
Synonyms Corticoid | Use Various | |
 | ||
Biological target Corticosteroid receptor | ||
Corticosteroids are a class of steroid hormones that are produced in the adrenal cortex of vertebrates, as well as the synthetic analogues of these hormones. Two main classes of corticosteroids, glucocorticoids and mineralocorticoids, are involved in a wide range of physiologic processes, including stress response, immune response, and regulation of inflammation, carbohydrate metabolism, protein catabolism, blood electrolyte levels, and behavior.
Contents
- Classes
- Medical uses
- Asthma
- Adverse effects
- Biosynthesis
- Chemical structure
- Group A Hydrocortisone type
- Group B Acetonides and related substances
- Group C Betamethasone type
- Group D Esters
- Topical steroids
- Inhaled steroids
- Oral forms
- Systemic forms
- History
- Name
- References
Some common naturally occurring steroid hormones are cortisol (C
21H
30O
5), corticosterone (C
21H
30O
4), cortisone (C
21H
28O
5) and aldosterone (C
21H
28O
5). (Note that aldosterone and cortisone share the same chemical formula but the structures are different.) The main corticosteroids produced by the adrenal cortex are cortisol and aldosterone.
Classes
Medical uses
Synthetic pharmaceutical drugs with corticosteroid-like effects are used in a variety of conditions, ranging from brain tumors to skin diseases. Dexamethasone and its derivatives are almost pure glucocorticoids, while prednisone and its derivatives have some mineralocorticoid action in addition to the glucocorticoid effect. Fludrocortisone (Florinef) is a synthetic mineralocorticoid. Hydrocortisone (cortisol) is typically used for replacement therapy, e.g. for adrenal insufficiency and congenital adrenal hyperplasia.
Medical conditions treated with systemic corticosteroids:
Topical formulations are also available for the skin, eyes (uveitis), lungs (asthma), nose (rhinitis), and bowels. Corticosteroids are also used supportively to prevent nausea, often in combination with 5-HT3 antagonists (e.g. ondansetron).
Typical undesired effects of glucocorticoids present quite uniformly as drug-induced Cushing's syndrome. Typical mineralocorticoid side-effects are hypertension (abnormally high blood pressure), hypokalemia (low potassium levels in the blood), hypernatremia (high sodium levels in the blood) without causing peripheral edema, metabolic alkalosis and connective tissue weakness. There may also be impaired wound healing or ulcer formation because of the immunosuppressive effects.
Clinical and experimental evidence indicates that corticosteroids can cause permanent eye damage by inducing central serous retinopathy (CSR, also known as central serous chorioretinopathy, CSC). A variety of steroid medications, from anti-allergy nasal sprays (Nasonex, Flonase) to topical skin creams, to eye drops (Tobradex), to prednisone have been implicated in the development of CSR.
Corticosteroids have been widely used in treating people with traumatic brain injury. A systematic review identified 20 randomised controlled trials and included 12,303 participants, then compared patients who received corticosteroids with patients who received no treatment. The authors recommended people with traumatic head injury should not be routinely treated with corticosteroids.
Asthma
There is some basis for genetic variation in patients' response to inhaled corticosteroids. Two genes of interest are CHRH1 (corticotropin-releasing hormone receptor 1) and TBX21 (transcription factor T-bet). Both genes display some degree of polymorphic variation in humans, which may explain how some patients respond better to inhaled corticosteroid therapy than others.
Adverse effects
Use of corticosteroids has numerous side-effects, some of which may be severe:
Biosynthesis
The corticosteroids are synthesized from cholesterol within the adrenal cortex. Most steroidogenic reactions are catalysed by enzymes of the cytochrome P450 family. They are located within the mitochondria and require adrenodoxin as a cofactor (except 21-hydroxylase and 17α-hydroxylase).
Aldosterone and corticosterone share the first part of their biosynthetic pathway. The last part is mediated either by the aldosterone synthase (for aldosterone) or by the 11β-hydroxylase (for corticosterone). These enzymes are nearly identical (they share 11β-hydroxylation and 18-hydroxylation functions), but aldosterone synthase is also able to perform an 18-oxidation. Moreover, aldosterone synthase is found within the zona glomerulosa at the outer edge of the adrenal cortex; 11β-hydroxylase is found in the zona fasciculata and zona glomerulosa.
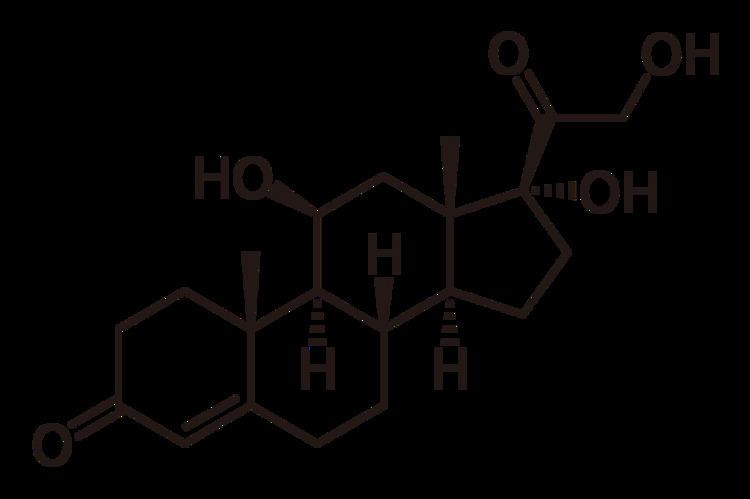
Chemical structure
In general, corticosteroids are grouped into four classes, based on chemical structure. Allergic reactions to one member of a class typically indicate an intolerance of all members of the class. This is known as the "Coopman classification", after S. Coopman, who defined this classification in 1989.
The highlighted steroids are often used in the screening of allergies to topical steroids.
Group A — Hydrocortisone type
Hydrocortisone, methylprednisolone, prednisolone, prednisone, and triamcinolone (short- to medium-acting glucocorticoids).
Group B — Acetonides (and related substances)
Amcinonide, budesonide, desonide, fluocinolone acetonide, fluocinonide, halcinonide, and triamcinolone acetonide.
Group C — Betamethasone type
Beclometasone, betamethasone, dexamethasone, fluocortolone, halometasone, and mometasone.
Group D — Esters
Group D1 — Halogenated (less labile)
Alclometasone dipropionate, betamethasone dipropionate, betamethasone valerate, clobetasol propionate, clobetasone butyrate, fluprednidene acetate, and mometasone furoate.
Group D2 — Labile prodrug esters
Ciclesonide, cortisone acetate, hydrocortisone aceponate, hydrocortisone acetate, hydrocortisone buteprate, hydrocortisone butyrate, hydrocortisone valerate, prednicarbate, and tixocortol pivalate.
Topical steroids
For use topically on the skin, eye, and mucous membranes.
Topical corticosteroids are divided in potency classes I to IV in most countries (A to D in Japan). There are seven categories used in the United States.
Inhaled steroids
for use to treat the nasal mucosa, sinuses, bronchii, and lungs. This group includes:
There is also a combination preparation containing fluticasone propionate and salmeterol xinafoate (a long-acting bronchodilator). It is approved for children over 12 years old.
Oral forms
Such as prednisone and prednisolone.
Systemic forms
Available in injectables for intravenous and parenteral routes.
History
First known use was in 1944. Tadeusz Reichstein together with Edward Calvin Kendall and Philip Showalter Hench were awarded the Nobel Prize for Physiology and Medicine in 1950 for their work on hormones of the adrenal cortex, which culminated in the isolation of cortisone.
Initially hailed as a miracle cure and liberally prescribed during the 1950s, steroid treatment brought about adverse events of such a magnitude that the next major category of anti-inflammatory drugs, the NSAID, was so named in order to demarcate from the opprobrium.
Corticosteroids have been used as drug treatment for some time. Lewis Sarett of Merck & Co. was the first to synthesize cortisone, using a complicated 36-step process that started with deoxycholic acid, which was extracted from ox bile. The low efficiency of converting deoxycholic acid into cortisone led to a cost of US $200 per gram. Russell Marker, at Syntex, discovered a much cheaper and more convenient starting material, diosgenin from wild Mexican yams. His conversion of diosgenin into progesterone by a four-step process now known as Marker degradation was an important step in mass production of all steroidal hormones, including cortisone and chemicals used in hormonal contraception. In 1952, D.H. Peterson and H.C. Murray of Upjohn developed a process that used Rhizopus mold to oxidize progesterone into a compound that was readily converted to cortisone. The ability to cheaply synthesize large quantities of cortisone from the diosgenin in yams resulted in a rapid drop in price to US $6 per gram, falling to $0.46 per gram by 1980. Percy Julian's research also aided progress in the field. The exact nature of cortisone's anti-inflammatory action remained a mystery for years after, however, until the leukocyte adhesion cascade and the role of phospholipase A2 in the production of prostaglandins and leukotrienes was fully understood in the early 1980s.
Corticosteroids were voted Allergen of the Year in 2005 by the American Contact Dermatitis Society.
Name
The cortico- part of the name refers to the adrenal cortex, which makes these steroid hormones. Thus a corticosteroid is a "cortex steroid".