
Specialty Internal medicine ICD-9-CM 276.0 eMedicine emerg/263 | ICD-10 E87.0 DiseasesDB 6266 Patient UK Hypernatremia | |
 | ||
Hypernatremia, also spelled hypernatraemia, is a high sodium ion level in the blood. Early symptoms may include a strong feeling of thirst, weakness, nausea, and loss of appetite. Severe symptoms include confusion, muscle twitching, and bleeding in or around the brain. Normal serum sodium levels are 135 - 145 mmol/L (135 - 145 mEq/L). Hypernatremia is generally defined as a serum sodium level of more than 145 mmol/L. Severe symptoms typically only occur when levels are above 160 mmol/L.
Contents
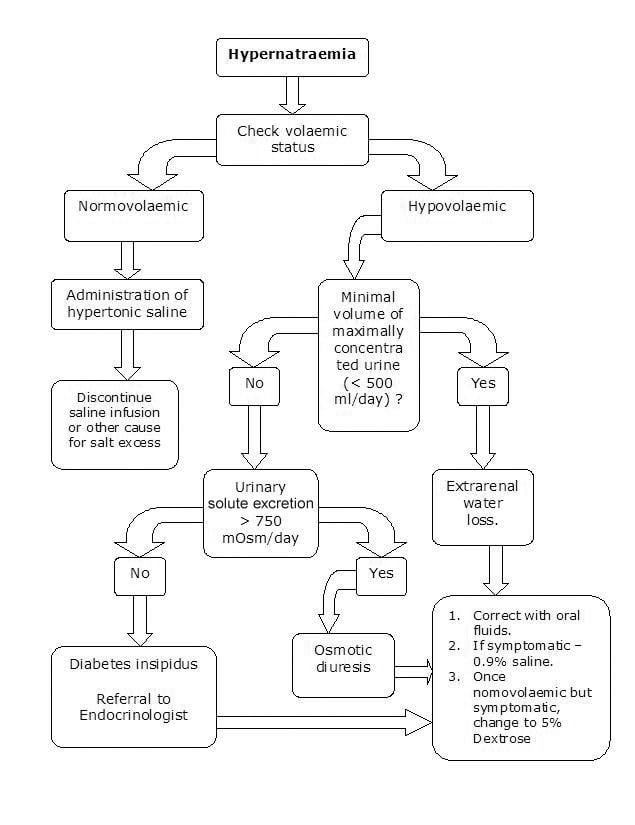
Hypernatremia is typically classified by a person's fluid status into low volume, normal volume, and high volume. Low volume hypernatremia can occur from sweating, vomiting, diarrhea, diuretic medication, or kidney disease. Normal volume hypernatremia can be due to fever, inappropriately decreased thirst, prolonged increased breath rate, diabetes insipidus, and from lithium among other causes. High volume hypernatremia can be due to hyperaldosteronism, be health care caused such as when too much intravenous 3% normal saline or sodium bicarbonate is given, or rarely be from eating too much salt. Low blood protein levels can result in a falsely high sodium measurement. The cause can usually be determined by the history of events. Testing the urine can help if the cause is unclear.
If the onset of hypernatremia was over a few hours, then it can be corrected relatively quickly using intravenous normal saline and 5% dextrose. Otherwise correction should occur slowly with, for those unable to drink water, half-normal saline. Hypernatremia due to diabetes insipidus as a result of a brain disorder, may be treated with the medication desmopressin. If the diabetes insipidus is due to kidney problems the medication which is causing it may need to be stopped. Hypernatremia affects 0.3-1% of people in hospital. It most often occurs in babies, those with impaired mental status, and the elderly. Hypernatremia is associated with an increased risk of death but it is unclear if it is the cause.
Signs and symptoms
The major symptom is thirst. The most important signs result from brain cell shrinkage and include confusion, muscle twitching or spasms. With severe elevations, seizures and comas may occur.
Severe symptoms are usually due to acute elevation of the plasma sodium concentration to above 157 mmol/L (normal blood levels are generally about 135–145 mmol/L for adults and elderly). Values above 180 mmol/L are associated with a high mortality rate, particularly in adults. However, such high levels of sodium rarely occur without severe coexisting medical conditions. Serum sodium concentrations have ranged from 150–228 mmol/L in survivors of acute salt overdosage, while levels of 153–255 mmol/L have been observed in fatalities. Vitreous humor is considered to be a better postmortem specimen than postmortem serum for assessing sodium involvement in a death.
Cause
Common causes of hypernatremia include:
Low volume
In those with low volume or hypovolemia:
Normal volume
In those with normal volume or euvolemia:
High volume
In those with high volume or hypervolemia:
Treatment
The cornerstone of treatment is administration of free water to correct the relative water deficit. Water can be replaced orally or intravenously. Water alone cannot be administered intravenously (because of osmolarity issue), but rather can be given with addition to dextrose or saline infusion solutions. However, overly rapid correction of hypernatremia is potentially very dangerous. The body (in particular the brain) adapts to the higher sodium concentration. Rapidly lowering the sodium concentration with free water, once this adaptation has occurred, causes water to flow into brain cells and causes them to swell. This can lead to cerebral edema, potentially resulting in seizures, permanent brain damage, or death. Therefore, significant hypernatremia should be treated carefully by a physician or other medical professional with experience in treatment of electrolyte imbalance, specific treatment like ACE inhibitors in heart failure and corticosteroids in nephropathy also can be used.