
Specialty Critical care medicine ICD-9-CM 276.8 MedlinePlus 000479 | ICD-10 E87.6 DiseasesDB 6445 | |
 | ||
Synonyms hypopotassaemia, hypopotassemia | ||
Hypokalemia, also spelled hypokalaemia, is a low level of potassium (K+) in the blood serum. Normal potassium levels are between 3.5 and 5.0 mmol/L (3.5 and 5.0 mEq/L) with levels below 3.5 mmol/L defined as hypokalemia. Mildly low levels do not typically cause symptoms. Symptoms may include feeling tired, leg cramps, weakness, and constipation. It increases the risk of an abnormal heart rhythm such as bradycardia and cardiac arrest.
Contents
- Signs and symptoms
- Causes
- Inadequate potassium intake
- Gastrointestinal or skin loss
- Urinary loss
- Distribution away from extracellular fluid
- Other
- Pseudohypokalemia
- Pathophysiology
- Blood
- Electrocardiogram
- Treatment
- References
Causes of hypokalemia include diarrhea, medications like furosemide and steroids, dialysis, diabetes insipidus, hyperaldosteronism, hypomagnesemia, and not enough intake in the diet. It is classified as severe when levels are less than 2.5 mmol/L. Low levels can also be detected on an electrocardiogram (ECG). Hyperkalemia refers to a high level of potassium in the blood serum.
The speed at which potassium should be replaced depends on whether or not there are symptoms or ECG changes. Mildly low levels can be managed with changes in the diet. Potassium supplements can be either taken by mouth or intravenously. If given by intravenous, generally less than 20 mmol are given over an hour. High concentration solutions (>40 mmol/L) should be given in a central line if possible. Magnesium replacement may also be required.
Hypokalemia is one of the most common water–electrolyte imbalances. It affects about 20% of people admitted to hospital. The word "hypokalemia" is from hypo- means "under"; kalium meaning potassium, and -emia means "condition of the blood".
Signs and symptoms
Mild hypokalemia is often without symptoms, although it may cause elevation of blood pressure, and can provoke the development of an abnormal heart rhythm. Severe hypokalemia, with serum potassium concentrations of 2.5–3 meq/l (Nl: 3.5–5.0 meq/l), may cause muscle weakness, myalgia, tremor, and muscle cramps (owing to disturbed function of skeletal muscle), and constipation (from disturbed function of smooth muscle). With more severe hypokalemia, flaccid paralysis and hyporeflexia may result. Reports exist of rhabdomyolysis occurring with profound hypokalemia with serum potassium levels less than 2 meq/l. Respiratory depression from severe impairment of skeletal muscle function is found in many patients.
Causes
Hypokalemia can result from one or more of these medical conditions:
Inadequate potassium intake
Perhaps the most obvious cause is insufficient consumption of potassium (that is, a low-potassium diet) or starvation. However, without excessive potassium loss from the body, this is a rare cause of hypokalemia. Usually only seen in anorexia nervosa patients and people on a ketogenic diet.
Gastrointestinal or skin loss
A more common cause is excessive loss of potassium, often associated with heavy fluid losses that "flush" potassium out of the body. Typically, this is a consequence of diarrhea, excessive perspiration, or losses associated with muscle-crush injury, or surgical procedures. Vomiting can also cause hypokalemia, although not much potassium is lost from the vomitus. Rather, heavy urinary losses of K+ in the setting of postemetic bicarbonaturia force urinary potassium excretion (see Alkalosis below). Other GI causes include pancreatic fistulae and the presence of adenoma.
Urinary loss
Distribution away from extracellular fluid
Other
Pseudohypokalemia
Pathophysiology
About 98% of the body's potassium is found inside cells, with the remainder in the extracellular fluid including the blood. This concentration gradient is maintained principally by the Na+/K+ pump.
Potassium is essential for many body functions, including muscle and nerve activity. The electrochemical gradient of potassium between the intracellular and extracellular space is essential for nerve function; in particular, potassium is needed to repolarize the cell membrane to a resting state after an action potential has passed. Lower potassium levels in the extracellular space cause hyperpolarization of the resting membrane potential. This hyperpolarization is caused by the effect of the altered potassium gradient on resting membrane potential as defined by the Goldman equation. As a result, a greater than normal stimulus is required for depolarization of the membrane to initiate an action potential.
In the heart, hypokalemia causes hyperpolarization in the myocytes' resting membrane potential. The more negative membrane potentials in the atrium may cause arrhythmias because of more complete recovery from sodium-channel inactivation, making the triggering of an action potential less likely. In addition, the reduced extracellular potassium (paradoxically) inhibits the activity of the IKr potassium current and delays ventricular repolarization. This delayed repolarization may promote reentrant arrhythmias.
Blood
Normal potassium levels are between 3.5 and 5.0 mmol/L with levels below 3.5 mmol/L (less than 3.5 mEq/L) defined as hypokalemia.
Electrocardiogram
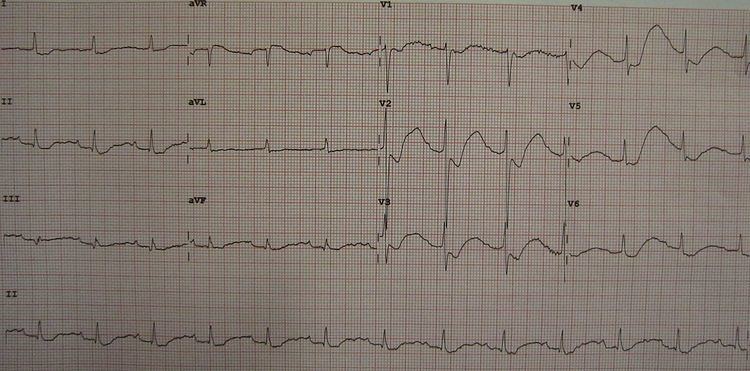
Some electrocardiographic (ECG) findings associated with hypokalemia include flattened or inverted T waves, a U wave, ST depression, and a wide PR interval. Due to prolonged repolarization of ventricular Purkinje fibers, a prominent U wave occurs, frequently superimposed upon the T wave and therefore produces the appearance of a prolonged QT interval.
Treatment
The most important treatment in severe hypokalemia is addressing the cause, such as improving the diet, treating diarrhea, or stopping an offending medication. Patients without a significant source of potassium loss and who show no symptoms of hypokalemia may not require treatment.
Mild hypokalemia (>3.0 meq/l) may be treated with oral potassium chloride supplements (Klor-Con, Sando-K, Slow-K). As this is often part of a poor nutritional intake, potassium-containing foods may be recommended, such as leafy green vegetables, avocados, tomatoes, coconut water, citrus fruits, oranges, or bananas. Both dietary and pharmaceutical supplements are used for people taking diuretic medications.
Severe hypokalemia (<3.0 meq/l) may require intravenous supplementation. Typically, a saline solution is used, with 20–40 meq/l KCl per liter over 3–4 hours. Giving IV potassium at faster rates (20–25 meq/hr) may predispose to ventricular tachycardias and requires intensive monitoring. A generally safe rate is 10 meq/hr. Even in severe hypokalemia, oral supplementation is preferred given its safety profile. Sustained-release formulations should be avoided in acute settings.
Difficult or resistant cases of hypokalemia may be amenable to a potassium-sparing diuretic, such as amiloride, triamterene, spironolactone, or eplerenone. Concomittant hypomagnesemia will inhibit potassium replacement, as magnesium is a cofactor for potassium uptake.
When replacing potassium intravenously, infusion by a central line is encouraged to avoid the frequent occurrence of a burning sensation at the site of a peripheral infusion, or the rare occurrence of damage to the vein. When peripheral infusions are necessary, the burning can be reduced by diluting the potassium in larger amounts of fluid, or mixing 3 ml of 1% lidocaine to each 10 meq of KCl per 50 ml of fluid. The practice of adding lidocaine, however, raises the likelihood of serious medical errors.