
ICD-10 L10.0 DiseasesDB 9764 | OMIM 169610 MedlinePlus 000882 | |
 | ||
Pemphigus vulgaris is a rare chronic blistering skin disease. It is classified as a type II hypersensitivity reaction, with the formation of antibodies against desmosomes, components of the skin that function to keep certain layers of skin bound to each other. As desmosomes are attacked, the layers of skin separate and the clinical picture resembles a blister. Over time the condition inevitably progresses without treatment: lesions increase in size and distribution throughout the body, behaving physiologically like a severe burn. Before the advent of modern treatments, mortality for the disease was close to 90%. Today, the mortality rate with treatment is between 5-15%.
Contents
Symptoms
Discrete, flaccid,bullae arising over normal skin,scalp,chest,back intertriginious areas ,Nikolsky and Bulla spread is +ve.
Pathophysiology
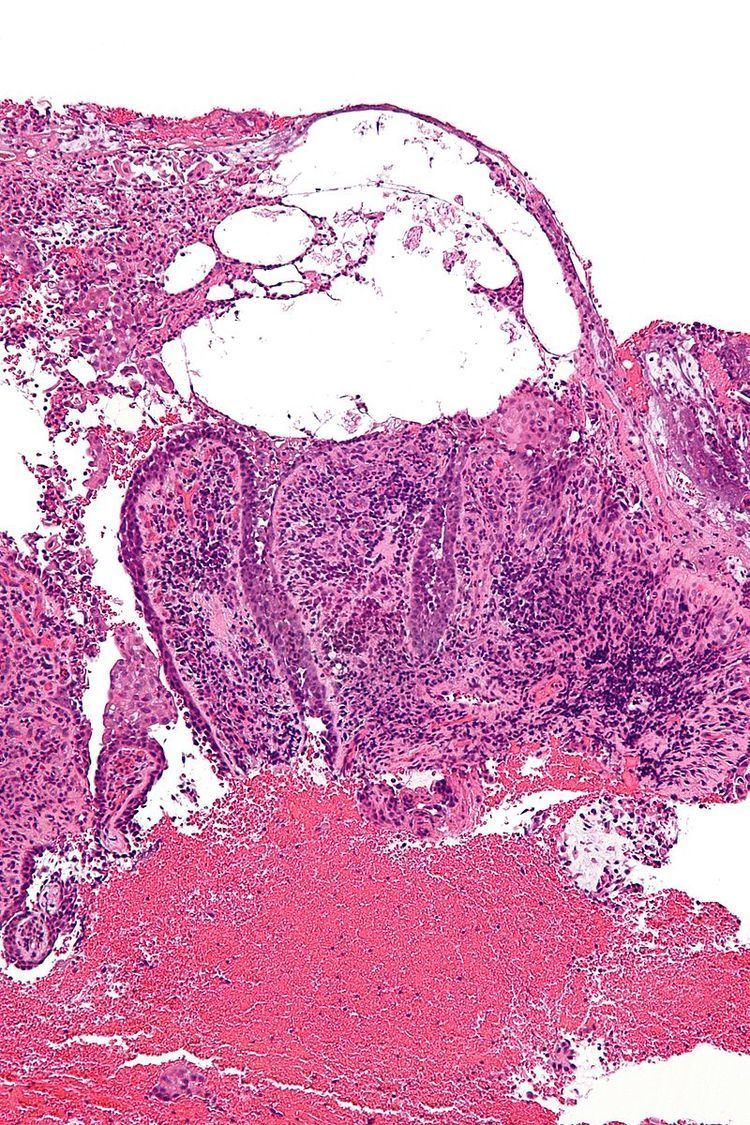
Pemphigus is an autoimmune disease caused by antibodies directed against both desmoglein 1 and desmoglein 3 present in desmosomes. Loss of desmosomes results in loss of cohesion between keratinocytes in the epidermis, and a disruption of the barrier function served by intact skin. The process is classified as a type II hypersensitivity reaction (in which antibodies bind to antigens on the body's own tissues). On histology, the basal keratinocytes are usually still attached to the basement membrane leading to a characteristic appearance called "tombstoning." Transudative fluid accumulates in between the keratinocytes and the basal layer (suprabasal split), forming a blister and resulting in what is known as a positive Nikolsky's sign. This is a contrasting feature from bullous pemphigoid, which is thought to be due to anti-hemidesmosome antibodies, and where the detachment occurs between the epidermis and dermis (subepidermal bullae). Clinically, pemphigus vulgaris is characterized by extensive flaccid blisters and mucocutaneous erosions. The severity of the disease, as well as the mucosal lesions, is believed to be directly proportional to the levels of desmoglein 3. Milder forms of pemphigus (like foliacious and erythematoses) are more anti-desmoglein 1 heavy.
The disease arises most often in middle-aged or older people, usually starting with a blister that ruptures easily. It can also start with blisters in the mouth. The lesions can become quite extensive.
Diagnosis
Because it is a rare disease, diagnosis is often complicated and takes a long time. Early in the disease patients may have erosions in the mouth or blisters on the skin. These blisters can be itchy or painful. Theoretically, the blisters should demonstrate a positive Nikolsky's sign, in which the skin sloughs off from slight rubbing, but this is not always reliable. The gold standard for diagnosis is a punch biopsy from the area around the lesion that is examined by direct immunofluorescent staining, in which cells are acantholytic, that is, lacking the normal intercellular connections that hold them together. These can also be seen on a Tzanck smear. These cells are basically rounded, nucleated keratinocytes formed due to antibody mediated damage to cell adhesion protein desmoglein.
Pemphigus vulgaris is easily confused with impetigo and candidiasis. IgG4 is considered pathogenic. The diagnosis can be confirmed by testing for the infections that cause these other conditions, and by a lack of response to antibiotic treatment. Eosinophils tend to be found within the blisters and provide an important clue supporting bullous pemphigoid as the diagnosis.
Treatment
Corticosteroids and other immunosuppressive drugs have historically been employed to reduce symptoms of pemphigus, yet steroids are associated with serious and long-lasting side effects and their use should be limited as much as possible. IVIg, mycophenolate mofetil, methotrexate, azathioprine, and cyclophosphamide have also been used with varying degrees of success.
An established alternative to steroids are monoclonal antibodies such as rituximab, which are increasingly being used as first line treatment. In numerous case series, many patients achieve remission after one cycle of rituximab. Treatment is more successful if initiated early on in the course of disease, perhaps even at diagnosis. Rituximab treatment combined with monthly IV immune globulin infusion has resulted in long-term remission with no recurrence of disease in 10 years after treatment was halted. This was a small trial study of 11 patients with 10 patients followed to completion.
Research into using genetically modified T-cells to treat pemphigus vulgaris in mice was reported in 2016 and holds promise as a potential curative therapy. Rituximab indiscriminately attacks all B cells, which reduces the body's ability to control infections. In the experimental treatment, human T cells are genetically engineered to recognize only those B cells that produce antibodies to desmoglein 3.