
ICD-10 J30 OMIM 607154 | Specialty Allergy and immunology ICD-9-CM 477 DiseasesDB 31140 | |
 | ||
Allergic rhinitis, also known as hay fever, is a type of inflammation in the nose which occurs when the immune system overreacts to allergens in the air. Signs and symptoms include a runny or stuffy nose, sneezing, red, itchy, and watery eyes, and swelling around the eyes. The fluid from the nose is usually clear. Symptom onset is often within minutes following exposure and they can affect sleep, the ability to work, and the ability to concentrate at school. Those whose symptoms are due to pollen typically develop symptoms during specific times of the year. Many people with allergic rhinitis also have asthma, allergic conjunctivitis, or atopic dermatitis.
Contents
- Signs and symptoms
- Cause
- Diagnosis
- Classification
- Local allergic rhinitis
- Prevention
- Treatment
- Antihistamines
- Steroids
- Other
- Allergen immunotherapy
- Alternative medicine
- Epidemiology
- History
- References
Allergic rhinitis is typically triggered by environmental allergens such as pollen, pet hair, dust, or mold. Inherited genetics and environmental exposures contribute to the development of allergies. Growing up on a farm and having multiple siblings decreases the risk. The underlying mechanism involves IgE antibodies attaching to the allergen and causing the release of inflammatory chemicals such as histamine from mast cells. Diagnosis is usually based on a medical history in combination with a skin prick test or blood tests for allergen-specific IgE antibodies. These tests, however, are sometimes falsely positive. The symptoms of allergies resemble those of the common cold; however, they often last for more than two weeks and typically do not include a fever.
Exposure to animals in early life might reduce the risk of developing allergies to them later. A number of medications may improve symptoms including nasal steroids, antihistamines such as diphenhydramine, cromolyn sodium, and leukotriene receptor antagonists such as montelukast. Medications are, however, not sufficient or are associated with side effects in many people. Exposing people to larger and larger amounts of allergen, known as allergen immunotherapy is often effective. The allergen may be given as injections just under the skin or as a tablet under the tongue. Treatment typically lasts three to five years after which benefits may be prolonged.
Allergic rhinitis is the type of allergy that affects the greatest number of people. In Western countries, between 10–30% of people are affected in a given year. It is most common between the ages of twenty and forty. The first accurate description is from the 10th century physician Rhazes. Pollen was identified as the cause in 1859 by Charles Blackley. In 1906 the mechanism was determined by Clemens von Pirquet. The link with hay came about due to an early (and incorrect) theory that the symptoms were brought about by the smell of new hay.
Signs and symptoms
The characteristic symptoms of allergic rhinitis are: rhinorrhea (excess nasal secretion), itching, sneezing fits, and nasal congestion and obstruction. Characteristic physical findings include conjunctival swelling and erythema, eyelid swelling, lower eyelid venous stasis (rings under the eyes known as "allergic shiners"), swollen nasal turbinates, and middle ear effusion.
There can also be behavioural signs; in order to relieve the irritation or flow of mucus, people may wipe or rub their nose with the palm of their hand in an upward motion: an action known as the "nasal salute" or the "allergic salute". This may result in a crease running across the nose (or above each nostril if only one side of the nose is wiped at a time), commonly referred to as the "transverse nasal crease", and can lead to permanent physical deformity if repeated enough.
People might also find that cross-reactivity occurs. For example, someone allergic to birch pollen may also find that he/she has an allergic reaction to the skin of apples or potatoes. A clear sign of this is the occurrence of an itchy throat after eating an apple or sneezing when peeling potatoes or apples. This occurs because of similarities in the proteins of the pollen and the food. There are many cross-reacting substances. Hay fever is not a true fever, meaning it does not cause a core body temperature in the fever over 37.5–38.3 °C (99.5-100.9 °F).
Cause
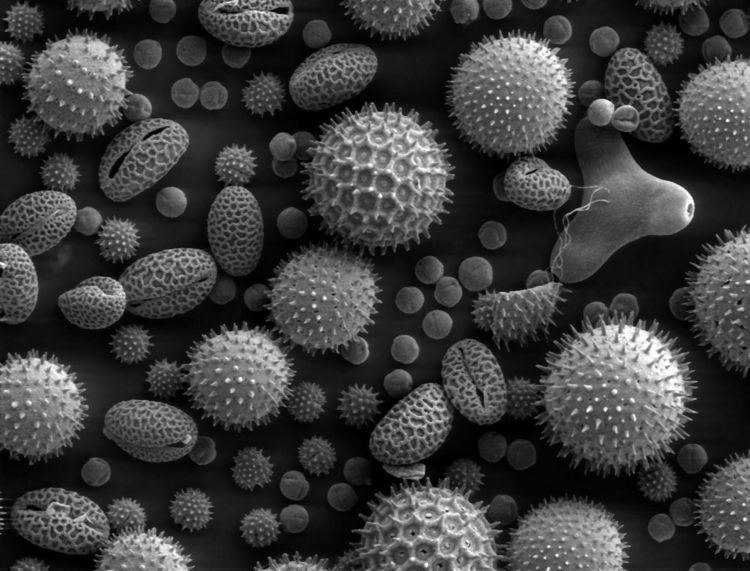
Allergic rhinitis triggered by the pollens of specific seasonal plants is commonly known as "hay fever", because it is most prevalent during haying season. However, it is possible to have allergic rhinitis throughout the year. The pollen that causes hay fever varies between individuals and from region to region; in general, the tiny, hardly visible pollens of wind-pollinated plants are the predominant cause. Pollens of insect-pollinated plants are too large to remain airborne and pose no risk. Examples of plants commonly responsible for hay fever include:
Allergic rhinitis may also be caused by allergy to Balsam of Peru, which is in various fragrances and other products.
Diagnosis
Allergy testing may reveal the specific allergens to which an individual is sensitive. Skin testing is the most common method of allergy testing. This may include a patch test to determine if a particular substance is causing the rhinitis, or an intradermal, scratch, or other test. Less commonly, the suspected allergen is dissolved and dropped onto the lower eyelid as a means of testing for allergies. This test should be done only by a physician, since it can be harmful if done improperly. In some individuals not able to undergo skin testing (as determined by the doctor), the RAST blood test may be helpful in determining specific allergen sensitivity. Peripheral eosinophilia can be seen in differential leukocyte count.
Allergy testing can either show allergies that are not actually causing symptoms or miss allergies that do cause symptoms. The intradermal allergy test is more sensitive than the skin prick test but is more often positive in people that do not have symptoms to that allergen.
Even if a person has negative skin-prick, intradermal and blood tests for allergies, he/she may still have allergic rhinitis, from a local allergy in the nose. This is called local allergic rhinitis. Specialized testing is necessary to diagnose local allergic rhinitis.
Classification
Allergic rhinitis may be seasonal or perennial. Seasonal allergic rhinitis occurs in particular during pollen seasons. It does not usually develop until after 6 years of age. Perennial allergic rhinitis occurs throughout the year. This type of allergic rhinitis is commonly seen in younger children.
Allergic rhinitis may also be classified as Mild-Intermittent, Moderate-Severe intermittent, Mild-Persistent, and Moderate-Severe Persistent. Intermittent is when the symptoms occur <4 days per week or <4 consecutive weeks. Persistent is when symptoms occur >4 days/week and >4 consecutive weeks. The symptoms are considered mild with normal sleep, no impairment of daily activities, no impairment of work or school, and if symptoms are not troublesome. Severe symptoms result in sleep disturbance, impairment of daily activities, and impairment of school or work.
Local allergic rhinitis
Local allergic rhinitis is an allergic reaction in the nose to an allergen, without systemic allergies. So skin-prick and blood tests for allergy are negative, but there are IgE antibodies produced in the nose that react to a specific allergen. Intradermal skin testing may also be negative.
The symptoms of local allergic rhinitis are the same as the symptoms of allergic rhinitis, including symptoms in the eyes. Just as with allergic rhinitis, people can have either seasonal or perennial local allergic rhinitis. The symptoms of local allergic rhinitis can be mild, moderate, or severe. Local allergic rhinitis is associated with conjunctivitis and asthma.
In one study, about 25% of people with rhinitis had local allergic rhinitis. In several studies, over 40% of people having been diagnosed with nonallergic rhinitis were found to actually have local allergic rhinitis. Steroid nasal sprays and oral antihistamines have been found to be effective for local allergic rhinitis.
Prevention
One way to prevent allergic rhinitis is to wear a respirator or mask when near potential allergens.
Growing up on a farm and having multiple brothers and or sisters decreases the risk.
Treatment
The goal of rhinitis treatment is to prevent or reduce the symptoms caused by the inflammation of affected tissues. Measures that are effective include avoiding the allergen. Intranasal corticosteroids are the preferred treatment if medications are required, with other options used only if these are not effective. Mite-proof covers, air filters, and withholding certain foods in childhood do not have evidence supporting their effectiveness.
Antihistamines
Antihistamine drugs can be taken orally and nasally to control symptoms such as sneezing, rhinorrhea, itching, and conjunctivitis.
It is best to take oral antihistamine medication before exposure, especially for seasonal allergic rhinitis. In the case of nasal antihistamines like azelastine antihistamine nasal spray, relief from symptoms is experienced within 15 minutes allowing for a more immediate 'as-needed' approach to dosage.
Ophthalmic antihistamines (such as azelastine in eye drop form and ketotifen) are used for conjunctivitis, while intranasal forms are used mainly for sneezing, rhinorrhea, and nasal pruritus.
Antihistamine drugs can have undesirable side-effects, the most notable one being drowsiness in the case of oral antihistamine tablets. First-generation antihistamine drugs such as diphenhydramine cause drowsiness, but second- and third-generation antihistamines such as cetirizine and loratadine are less likely to cause this problem.
Pseudoephedrine is also indicated for vasomotor rhinitis. It is used only when nasal congestion is present and can be used with antihistamines. In the United States, oral decongestants containing pseudoephedrine must be purchased behind the pharmacy counter by law in effort to prevent the making of methamphetamine.
Steroids
Intranasal corticosteroids are used to control symptoms associated with sneezing, rhinorrhea, itching, and nasal congestion. Steroid nasal sprays are effective and safe, and may be effective without oral antihistamines. They take several days to act and so must be taken continually for several weeks, as their therapeutic effect builds up with time.
In 2013, a study compared the efficacy of mometasone furoate nasal spray to betamethasone oral tablets for the treatment of people with seasonal allergic rhinitis and found that the two have virtually equivalent effects on nasal symptoms in people.
Systemic steroids such as prednisone tablets and intramuscular triamcinolone acetonide or glucocorticoid (such as betamethasone) injection are effective at reducing nasal inflammation, but their use is limited by their short duration of effect and the side-effects of prolonged steroid therapy.
Other
Other measures that may be used second line include: decongestants, cromolyn, leukotriene receptor antagonists, and nonpharmacologic therapies such as nasal irrigation.
Topical decongestants may also be helpful in reducing symptoms such as nasal congestion, but should not be used for long periods, as stopping them after protracted use can lead to a rebound nasal congestion called rhinitis medicamentosa.
For nocturnal symptoms, intranasal corticosteroids can be combined with nightly oxymetazoline, an adrenergic alpha-agonist, or an antihistamine nasal spray without risk of rhinitis medicamentosa.
Allergen immunotherapy
Allergen immunotherapy (AIT, also termed desensitization) treatment involves administering doses of allergens to accustom the body to substances that are generally harmless (pollen, house dust mites), thereby inducing specific long-term tolerance. Allergy immunotherapy can be administered orally (as sublingual tablets or sublingual drops), or by injections under the skin (subcutaneous).
Alternative medicine
Therapeutic efficacy of alternative treatments such as acupuncture and homeopathy is not supported by available evidence. Some evidence shows that acupuncture is effective for rhinitis, whereas other evidence does not. The overall quality of evidence, however, is poor.
Epidemiology
Allergic rhinitis is the type of allergy that affects the greatest number of people. In Western countries, between 10 and 30 percent of people are affected in a given year. It is most common between the ages of twenty and forty.
History
The first accurate description is from the 10th century physician Rhazes. Pollen was identified as the cause in 1859 by Charles Blackley. While in 1906 the mechanism was determined by Clemens von Pirquet. The link with hay came about due to an early (and incorrect) theory that the symptoms were brought about by the smell of new hay.