
ICD-9-CM 364 MedlinePlus 001005 | ICD-10 H20 DiseasesDB 13676 eMedicine oph/580 emerg/284 | |
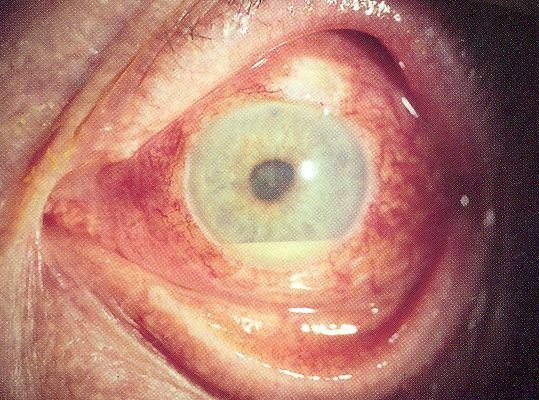 | ||
Uveitis is the inflammation of the uvea, the pigmented layer that lies between the inner retina and the outer fibrous layer composed of the sclera and cornea. The uvea consists of the middle layer of pigmented vascular structures of the eye and includes the iris, ciliary body, and choroid. Uveitis is an ophthalmic emergency and requires a thorough examination by an optometrist or ophthalmologist and urgent treatment to control the inflammation.
Contents
- Classification
- Anterior uveitis
- Intermediate uveitis
- Posterior uveitis
- Causes
- Noninfectious or autoimmune causes
- Infectious causes
- Associated with systemic diseases
- Drug related side effects
- White Dot syndromes
- Masquerade syndromes
- Immunologic factors
- Genetic factors
- Infectious agents
- Diagnosis
- Treatment
- Prognosis
- Epidemiology
- References
Classification
Uveitis is classified anatomically into anterior, intermediate, posterior, and panuveitic forms—based on the part of the eye primarily affected. Prior to the twentieth century, uveitis was typically referred to in English as "ophthalmia."
Anterior uveitis
Intermediate uveitis
Most common:
Intermediate uveitis normally only affects one eye. Less common is the presence of pain and photophobia.
Posterior uveitis
Inflammation in the back of the eye is commonly characterized by:
Causes
Uveitis is usually an isolated illness, but can be associated with many other medical conditions.
In anterior uveitis, no associated condition or syndrome is found in approximately one-half of cases. However, anterior uveitis is often one of the syndromes associated with HLA-B27. Presence this type of HLA allele has a relative risk of evolving this disease by approximately 15%.
The most common form of uveitis is acute anterior uveitis (AAU). It is most commonly associated with HLA-B27, which has important features: HLA-B27 AAU can be associated with ocular inflammation alone or in association with systemic disease. HLA-B27 AAU has characteristic clinical features including male preponderance, unilateral alternating acute onset, a non-granulomatous appearance, and frequent recurrences whereas HLA-B27 negative AAU has an equivalent male to female onset, bilateral chronic course, and more frequent granulomatous appearance. Rheumatoid arthritis is not uncommon in Asian countries as a significant association of uveitis.
Noninfectious or autoimmune causes
Infectious causes
Uveitis may be an immune response to fight an infection inside the eye. While representing the minority of patients with uveitis, such possible infections include:
Associated with systemic diseases
Systemic disorders that can be associated with uveitis include:
Drug related side effects
White Dot syndromes
Occasionally, uveitis is not associated with a systemic condition: the inflammation is confined to the eye and has unknown cause. In some of these cases, the presentation in the eye is characteristic of a described syndrome, which are called white dot syndromes, and include the following diagnoses:
Masquerade syndromes
Masquerade syndromes are those conditions that include the presence of intraocular cells but are not due to immune-mediated uveitis entities. These may be divided into neoplastic and non-neoplastic conditions.
Immunologic factors
Onset of uveitis can broadly be described as a failure of the ocular immune system and the disease results from inflammation and tissue destruction. Uveitis is driven by the Th17 T cell sub-population that bear T-cell receptors specific for proteins found in the eye. These are often not deleted centrally whether due to ocular antigen not being presented in the thymus (therefore not negatively selected) or a state of anergy is induced to prevent self targeting.
Autoreactive T cells must normally be held in check by the suppressive environment produced by microglia and dendritic cells in the eye. These cells produce large amounts of TGF beta and other suppressive cytokines, including IL-10, to prevent damage to the eye by reducing inflammation and causing T cells to differentiate to inducible T reg cells. Innate immune stimulation by bacteria and cellular stress is normally suppressed by myeloid suppression while inducible Treg cells prevent activation and clonal expansion of the autoreactive Th1 and Th17 cells that possess potential to cause damage to the eye.
Whether through infection or other causes, this balance can be upset and autoreactive T cells allowed to proliferate and migrate to the eye. Upon entry to the eye, these cells may be returned to an inducible Treg state by the presence of IL-10 and TGF-beta from microglia. Failure of this mechanism leads to neutrophil and other leukocyte recruitment from the peripheral blood through IL-17 secretion. Tissue destruction is mediated by non-specific macrophage activation and the resulting cytokine cascades. Serum TNF-α is significantly elevated in cases while IL-6 and IL-8 are present in significantly higher quantities in the aqueous humour in patients with both quiescent and active uveitis. These are inflammatory markers that non-specifically activate local macrophages causing tissue damage.
Genetic factors
The cause of non-infectious uveitis is unknown but there are some strong genetic factors that predispose disease onset including HLA-B27 and the PTPN22 genotype.
Infectious agents
Recent evidence has pointed to reactivation of herpes simplex, varicella zoster and other viruses as important causes of developing what was previously described as idiopathic anterior uveitis. Bacterial infection is another significant contributing factor in developing uveitis.
Diagnosis
Diagnosis includes dilated fundus examination to rule out posterior uveitis, which presents with white spots across the retina along with retinitis and vasculitis.
Laboratory testing is usually used to diagnose specific underlying diseases, including rheumatologic tests (e.g. antinuclear antibody, rheumatoid factor, angiotensin converting enzyme inhibitor) and serology for infectious diseases (Syphilis, Toxoplasmosis, Tuberculosis).
Major histocompatibility antigen testing may be performed to investigate genetic susceptibility to uveitis. The most common antigens include HLA-B27, HLA-A29 (in birdshot chorioretinopathy) and HLA-B51 (in Behçet disease).
Radiology X-ray may be used to show coexisting arthritis and chest X-ray may be helpful in sarcoidosis.
Treatment
Uveitis is typically treated with glucocorticoid steroids, either as topical eye drops (prednisolone acetate) or as oral therapy. Prior to the administration of corticosteroids, corneal ulcers must be ruled out. This is typically done using a fluoresence dye test. In addition to corticosteroids, topical cycloplegics, such as atropine or homatropine, may be used. Successful treatment of active uveitis increases T-regulatory cells in the eye, which likely contributes to disease regression. In some cases an injection of posterior subtenon triamcinolone acetate may also be given to reduce the swelling of the eye.
Antimetabolite medications, such as methotrexate are often used for recalcitrant or more aggressive cases of uveitis. Experimental treatments with Infliximab or other anti-TNF infusions may prove helpful.
The anti-diabetic drug metformin is reported to inhibit the process that causes the inflammation in uveitis.
In the case of herpetic uveitis, anti-viral medications, such as valaciclovir or aciclovir, may be administered to treat the causative viral infection.
Prognosis
The prognosis is generally good for those who receive prompt diagnosis and treatment, but serious complication including cataracts, glaucoma, band keratopathy, macular edema and permanent vision loss may result if left untreated. The type of uveitis, as well as its severity, duration, and responsiveness to treatment or any associated illnesses, all factor into the outlook.
Epidemiology
Uveitis affects approximately 1 in 4500 people and is most common between the ages 20 to 60 with men and women affected equally.
In western countries, anterior uveitis accounts for between 50% and 90% of uveitis cases. In Asian countries the proportion is between 28% and 50%.
Uveitis is estimated to be responsible for approximately 10%-20% of the blindness in the United States.