
ICD-10 H33 DiseasesDB 11417 | ICD-9-CM 361 MedlinePlus 001027 | |
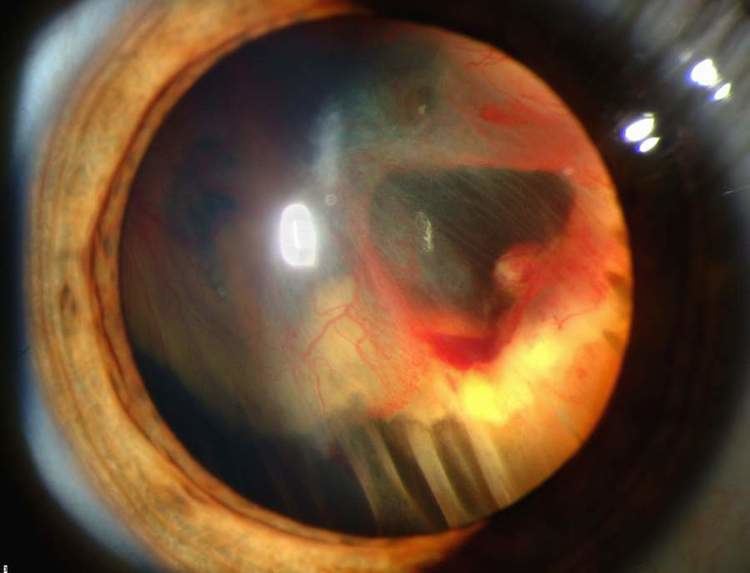 | ||
Retinal detachment is a disorder of the eye in which the retina separates from the layer underneath. Symptoms include an increase in the number of floaters, flashes of light, and worsening of the outer part of the visual field. This may be described as a curtain over part of the field of vision. In about 7% of cases both eyes are affected. Without treatment permanent loss of vision may occur.
Contents
- Signs and symptoms
- Risk factors
- Diagnosis
- Types
- Treatment
- Cryopexy and laser photocoagulation
- Scleral buckle surgery
- Pneumatic retinopexy
- Vitrectomy
- Prognosis
- Epidemiology
- References
The mechanism most commonly involves a break in the retina that then allows the fluid in the eye to get behind the retina. A break in the retina can occur from a posterior vitreous detachment, injury to the eye, or inflammation of the eye. Other risk factors include being short sighted and previous cataract surgery. Retinal detachments also rarely occur due to a choroidal tumor. Diagnosis is by either looking at the back of the eye with an ophthalmoscope or by ultrasound.
In those with a retinal tear, efforts to prevent it becoming a detachment include cryotherapy using a cold probe or photocoagulation using a laser. Treatment of retinal detachment should be carried out in a timely manner. This may include scleral buckling where silicone is sutured to the outside of the eye, pneumatic retinopexy where gas is injected into the eye, or vitrectomy where the vitreous is partly removed and replaced with either gas or oil.
Retinal detachments affect between 0.6 and 1.8 people per 10,000 per year. About 0.3% of people are affected at some point in their life. It is most common in people who are in their 60s or 70s. Males are more often affected than females. The long term outcomes depend on the duration of the detachment and whether the macula was detached. If treated before the macula detaches outcomes are generally good.
Signs and symptoms
A rhegmatogenous retinal detachment is commonly preceded by a posterior vitreous detachment which gives rise to these symptoms:
Although most posterior vitreous detachments do not progress to retinal detachments, those that do produce the following symptoms:
In the event of an appearance of sudden flashes of light or floaters, an eye doctor needs to be consulted immediately. A shower of floaters or any loss of vision, too, is a medical emergency.
Risk factors
Risk factors for retinal detachment include severe myopia, retinal tears, trauma, family history, as well as complications from cataract surgery.
Retinal detachment can be mitigated in some cases when the warning signs are caught early. The most effective means of prevention and risk reduction is through education of the initial signs, and encouragement for people to seek ophthalmic medical attention if they have symptoms suggestive of a posterior vitreous detachment. Early examination allows detection of retinal tears which can be treated with laser or cryotherapy. This reduces the risk of retinal detachment in those who have tears from around 1:3 to 1:20. For this reason, the governing bodies in some sports require regular eye examination.
Trauma-related cases of retinal detachment can occur in high-impact sports or in high speed sports. Although some recommend avoiding activities that increase pressure in the eye, including diving and skydiving, there is little evidence to support this recommendation, especially in the general population. Nevertheless, ophthalmologists generally advise people with high degrees of myopia to try to avoid exposure to activities that have the potential for trauma, increase pressure on or within the eye itself, or include rapid acceleration and deceleration, such as bungee jumping or roller coaster rides.
Intraocular pressure spikes occur during any activity accompanied by the Valsalva maneuver, including weightlifting. An epidemiological study suggests that heavy manual lifting at work may be associated with increased risk of rhegmatogenous retinal detachment, but this relationship is not strong. In this study, obesity also appeared to increase the risk of retinal detachment. A high Body Mass Index (BMI) and elevated blood pressure have been identified as a risk factor in non-myopic individuals.
Genetic factors promoting local inflammation and photoreceptor degeneration may also be involved in the development of the disease.
Other risk factors include the following:
Diagnosis
Retinal detachment can be examined by fundus photography or ophthalmoscopy. Fundus photography generally needs a considerably larger instrument than the ophthalmoscope, but has the advantage of availing the image to be examined by a specialist at another location and/or time, as well as providing photo documentation for future reference. Modern fundus photographs generally recreate considerably larger areas of the fundus than what can be seen at any one time with handheld ophthalmoscopes.
Ultrasound has diagnostic accuracy similar to that of examination by an ophthalmologist. The recent meta-analysis shows the diagnostic accuracy of emergency department (ED) ocular ultrasonography is high. The sensitivity and specificity ranged from 97% to 100% and 83% to 100%. The typical feature of retinal detachment when viewed on ultrasound is "flying angel sign". It shows the detached retina moving with a fixed point under the B mode, linear probe 10MHz.
Types
A minority of retinal detachments result from trauma, including blunt blows to the orbit, penetrating trauma, and concussions to the head. A retrospective Indian study of more than 500 cases of rhegmatogenous detachments found that 11% were due to trauma, and that gradual onset was the norm, with over 50% presenting more than one month after the inciting injury.
Treatment
There are several methods of treating a detached retina, each of which depends on finding and closing the breaks that have formed in the retina. All three of the procedures follow the same three general principles:
- Find all retinal breaks
- Seal all retinal breaks
- Relieve present (and future) vitreoretinal traction
Cryopexy and laser photocoagulation
Cryotherapy (freezing) or laser photocoagulation are occasionally used alone to wall off a small area of retinal detachment so that the detachment does not spread.
Scleral buckle surgery
Scleral buckle surgery is an established treatment in which the eye surgeon sews one or more silicone bands (or tyres) to the sclera (the white outer coat of the eyeball). The bands push the wall of the eye inward against the retinal hole, closing the break or reducing fluid flow through it and reducing the effect of vitreous traction thereby allowing the retina to re-attach. Cryotherapy (freezing) is applied around retinal breaks prior to placing the buckle. Often subretinal fluid is drained as part of the buckling procedure. The buckle remains in situ. The most common side effect of a scleral operation is myopic shift. That is, the operated eye will be more short sighted after the operation. Radial scleral buckle is indicated for U-shaped tears or Fishmouth tears, and posterior breaks. Circumferential scleral buckle is indicated for multiple breaks, anterior breaks and wide breaks. Encircling buckles are indicated for breaks covering more than 2 quadrants of retinal area, lattice degeneration located on more than 2 quadrant of retinal area, undetectable breaks, and proliferative vitreous retinopathy.
Pneumatic retinopexy
This operation is generally performed in the doctor's office under local anesthesia. It is another method of repairing a retinal detachment in which a gas bubble (SF6 or C3F8 gas) is injected into the eye after which laser or freezing treatment is applied to the retinal hole. The patient's head is then positioned so that the bubble rests against the retinal hole. Patients may have to keep their heads tilted for several days to keep the gas bubble in contact with the retinal hole. The surface tension of the gas/water interface seals the hole in the retina, and allows the retinal pigment epithelium to pump the subretinal space dry and "suck the retina back into place". This strict positioning requirement makes the treatment of the retinal holes and detachments that occurs in the lower part of the eyeball impractical. This procedure is usually combined with cryopexy or laser photocoagulation. Pneumatic retinopexy has significantly lower success rates compared to scleral buckle surgery and vitrectomy. Some initially successful cases will fail during the weeks and months after surgery. In some of the failed cases, an area of the retina which was healthy and attached prior to the initial pneumatic retinopexy repair procedure develops new tears and/or becomes detached. A recent Cochrane Review compared outcomes from patients receiving retinal reattachment from pneumatic retinopexy versus scleral buckle. Though the quality of evidence from two randomized controlled trials was low, eyes having received the pneumatic retinopexy procedure were more likely to have a recurrence of retinal detachment by follow-up, and were 11% less likely to achieve retinal reattachment, compared to scleral buckle.
Vitrectomy
Vitrectomy is an increasingly used treatment for retinal detachment. It involves the removal of the vitreous gel and is usually combined with filling the eye with either a gas bubble (SF6 or C3F8 gas) or silicone oil (PDMS). An advantage of using gas in this operation is that there is no myopic shift after the operation and gas is absorbed within a few weeks. PDMS, if used, needs to be removed after a period of 2–8 months depending on surgeon's preference. Silicone oil is more commonly used in cases associated with proliferative vitreo-retinopathy (PVR). A disadvantage is that a vitrectomy always leads to more rapid progression of a cataract in the operated eye. In many places vitrectomy is the most commonly performed operation for the treatment of retinal detachment. A recent Cochrane Review assessing various tamponade agents for patients with retinal detachment associated with PVR found that patients treated with C3F8 gas and standard silicone oil had visual and anatomic advantages over patients using SF6. Heavy silicone oil did not show any advantages over regular silicone oil.
Prognosis
85 percent of cases will be successfully treated with one operation with the remaining 15 percent requiring 2 or more operations. After treatment patients gradually regain their vision over a period of a few weeks, although the visual acuity may not be as good as it was prior to the detachment, particularly if the macula was involved in the area of the detachment.
Up until the early 20th century, the prognosis for rhegmatogenous retinal detachment was very poor, and no effective treatments were available. Currently, about 95 percent of cases of retinal detachment can be repaired successfully. Treatment failures usually involve either the failure to recognize all sites of detachment, the formation of new retinal breaks, or proliferative vitreoretinopathy.
Involvement of the macula portends a worse prognosis. In cases where the macula is not involved (detached), 90 percent of patients have 20/40 vision or better after reattachment surgery. Some damage to vision may occur during reattachment surgery, and 10 percent of patients with normal vision experience some vision loss after a successful reattachment surgery.
It is not clear if surgery is beneficial for asymptomatic retinal breaks or lattice degeneration.
Epidemiology
The incidence of retinal detachment in otherwise normal eyes is around 5 new cases in 100,000 persons per year. Detachment is more frequent in middle-aged or elderly populations, with rates of around 20 in 100,000 per year. The lifetime risk in normal individuals is about 1 in 300. Asymptomatic retinal breaks are present in about 6% of eyes in both clinical and autopsy studies.
Although retinal detachment usually occurs in just one eye, there is a 15% chance of it developing in the other eye, and this risk increases to 25–30% in patients who have had a retinal detachment and cataracts extracted from both eyes.