
Symbol IL17A Entrez 3605 OMIM 603149 | Alt. symbols IL17, CTLA8 HUGO 5981 RefSeq NP_002181 | |
 | ||
Interleukin 17A (IL-17 or IL-17A), originally identified as a transcript from a rodent T-cell hybridoma by Rouvier et al. in 1993, is the founding member of a group of cytokines called the IL-17 family. Known as CTLA8 in rodents, IL-17 shows high homology to viral IL-17 encoded by an open reading frame of the T-lymphotropic rhadinovirus Herpesvirus saimiri.
Contents
- Family members
- Function
- Gene expression
- Structure
- Role in Psoriasis
- Role in asthma
- Therapeutic target
- Receptors
- References
Interleukin 17 is a pro-inflammatory cytokine produced by T-helper cells and is induced by IL-23. To elicit its functions, IL-17 binds to a type I cell surface receptor called IL-17R of which there are at least three variants IL17RA, IL17RB, and IL17RC. IL-17 acts as a potent mediator in delayed-type reactions by increasing chemokine production in various tissues. Signaling from IL-17 recruits monocytes and neutrophils to the site of inflammation in response to invasion by pathogens, similar to Interferon gamma. In promoting inflammation, IL-17 has been demonstrated to act synergistically with tumor necrosis factor and interleukin-1. This activity can also be redirected towards the host and result in various autoimmune disorders that involve chronic inflammation, such as the skin disorder psoriasis.
Family members
In addition to IL-17A, members of the IL-17 family include IL-17B, IL-17C, IL-17D, IL-17E (also called IL-25), and IL-17F. All members of the IL-17 family have a similar protein structure, with four highly conserved cysteine residues critical to their 3-dimensional shape, yet they have no sequence similarity to any other known cytokines. Phylogenetic analysis reveals that among IL-17 family members, the IL-17F isoforms 1 and 2 (ML-1) have the highest homology to IL-17A (sharing 55 and 40% amino acid identity to IL-17A respectively), followed by IL-17B (29%), IL-17D (25%), IL-17C (23%), and IL-17E being most distantly related to IL-17A (17%). These cytokines are all well conserved in mammals, with as much as 62–88% of amino acids conserved between the human and mouse homologs.
Function
Numerous immune regulatory functions have been reported for the IL-17 family of cytokines, presumably due to their induction of many immune signaling molecules. The most notable role of IL-17 is its involvement in inducing and mediating proinflammatory responses. IL-17 is commonly associated with allergic responses. IL-17 induces the production of many other cytokines (such as IL-6, G-CSF, GM-CSF, IL-1β, TGF-β, TNF-α), chemokines (including IL-8, GRO-α, and MCP-1), and prostaglandins (e.g., PGE2) from many cell types (fibroblasts, endothelial cells, epithelial cells, keratinocytes, and macrophages). IL-17 acts with IL-22 (produced by T helper 17 cells) to induce expression of antimicrobial peptide by keratinocytes.
The release of cytokines causes many functions, such as airway remodeling, a characteristic of IL-17 responses. The increased expression of chemokines attracts other cells including neutrophils but not eosinophils. IL-17 function is also essential to a subset of CD4+ T-Cells called T helper 17 (Th17) cells. As a result of these roles, the IL-17 family has been linked to many immune/autoimmune related diseases including rheumatoid arthritis, asthma, lupus, allograft rejection, anti-tumour immunity and recently psoriasis and multiple sclerosis.
Gene expression
The gene for human IL-17 is 1874 base pairs long and was cloned from CD4+ T cells. Each member of the IL-17 family has a distinct pattern of cellular expression. The expression of IL-17A and IL-17F appear to be restricted to a small group of activated T cells, and upregulated during inflammation. IL-17B is expressed in several peripheral tissues and immune tissues. IL-17C is also highly upregulated in inflammatory conditions, although in resting conditions is low in abundance. IL-17D is highly expressed in the nervous system and in skeletal muscle and IL-17E is found at low levels in various peripheral tissues.
Much progress has been made in the understanding of the regulation of IL-17. At first, Aggarwal et al. showed that production of IL-17 was dependent on IL-23. Later, a Korean group discovered that STAT3 and NF-κB signalling pathways are required for this IL-23-mediated IL-17 production. Consistent with this finding, Chen et al. showed that another molecule, SOCS3, plays an important role in IL-17 production. In the absence of SOCS3, IL-23-induced STAT3 phosphorylation is enhanced, and phosphorylated STAT3 binds to the promotor regions of both IL-17A and IL-17F increasing their gene activity. In contrast, some scientists believe IL-17 induction is independent of IL-23. Several groups have identified ways to induce IL-17 production both in vitro and in vivo by distinct cytokines, called TGF-β and IL-6, without the need for IL-23. Although IL-23 is not required for IL-17 expression in this situation, IL-23 may play a role in promoting survival and/or proliferation of the IL-17 producing T-cells. Recently, Ivanov et al. found that the thymus specific nuclear receptor, ROR-γ, directs differentiation of IL-17-producing T cells.
Structure
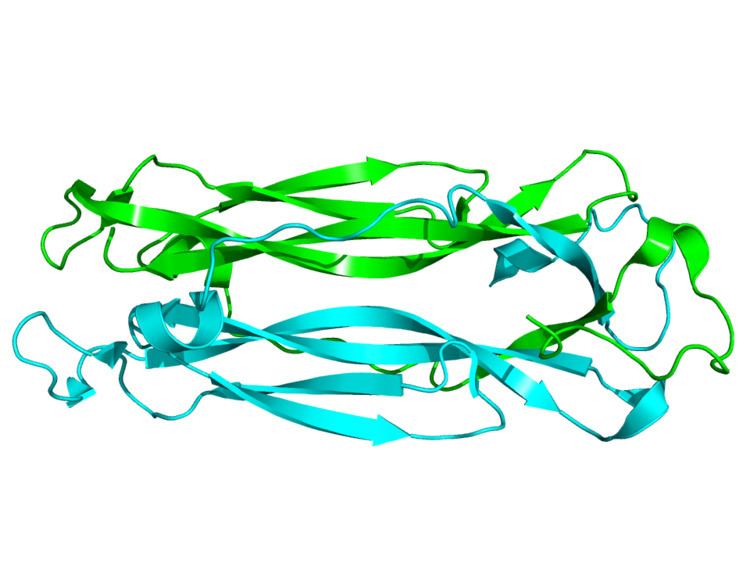
IL-17(A) is a 155-amino acid protein that is a disulfide-linked, homodimeric, secreted glycoprotein with a molecular mass of 35 kDa. Each subunit of the homodimer is approximately 15-20 KDa. The structure of IL-17 consists of a signal peptide of 23 amino acids (aa) followed by a 123-aa chain region characteristic of the IL-17 family. An N-linked glycosylation site on the protein was first identified after purification of the protein revealed two bands, one at 15 KDa and another at 20 KDa. Comparison of different members of the IL-17 family revealed four conserved cysteines that form two disulfide bonds. IL-17 is unique in that it bears no resemblance to other known interleukins. Furthermore, IL-17 bears no resemblance to any other known proteins or structural domains.
The crystal structure of IL-17F, which is 50% homologous to IL-17A, revealed that IL-17F is structurally similar to the cysteine knot family of proteins that includes the neurotrophins. The cysteine knot fold is characterized by two sets of paired β-strands stabilized by three disulfide interactions. However, in contrast to the other cysteine knot proteins, IL-17F lacks the third disulfide bond. Instead, a serine replaces the cysteine at this position. This unique feature is conserved in the other IL-17 family members. IL-17F also dimerizes in a fashion similar to nerve growth factor (NGF) and other neurotrophins.
Role in Psoriasis
Recent work suggests the IL-23/IL-17 pathway plays a major role in the autoimmune disorder psoriasis. In this condition, immune cells react to inflammatory molecules released within the skin around the joints and scalp. This response causes the epidermal cells to recycle more rapidly than usual, which leads to the formation of red, scaly lesions and chronic skin inflammation. Analysis of biopsies taken from lesions of psoriasis patients show an enrichment of cytotoxic T cells and neutrophils containing IL-17. This indicates an excessive infiltration of pro-inflammatory immune cells and IL-17 cytokines are associated with the development of psoriasis.
Studies conducted in mice demonstrate that removing either IL-23 or IL-17 decreases the progression of psoriasis. Mice injected with monoclonal antibodies targeting IL-17 blocked, or neutralized, down stream signaling of this cytokine and decreased epidermal hyperplasia. Similarly, genetically modifying mice to not express IL-23 or IL-17 receptors significantly reduced psoriatic lesion development upon stimulation with the lesion-causing tumor promoter 12-O-tetradecanoylphorbol-13-acetate.
IL-17 promotes psoriasis by contributing to the inflammatory response that damages and overturns the keratinocyte cells of the epidermal layer. Inflammation begins with keratinocyte cells entering the final stages of their cell cycle, which activates immature dendritic cells (DC). Cytokines released from DCs stimulate dying keratinocytes to secrete TNF-alpha, IL-1 and IL-6 leading to the chemotaxis of T cells, natural killer cells and monocytes to the epidermis. These cells release IL-23 which induce Th17 cells to produce IL-17.
IL-17 interaction with IL-17RA receptors, abundant on the keratinocyte cell surface, incite epidermal cells to increase expression of IL-6, antimicrobial peptides, IL-8 and CCL20. Increased concentration of IL-6 alters the epidermal environment by decreasing the ability of T regulatory cells to control the behavior of Th17 cells. Reduced regulation allows uninhibited proliferation of Th17 cells and production of IL-17 in psoriatic lesions, augmenting IL-17 signaling. Antimicrobial peptides and IL-8 attract neutrophils to the site of injury where these cells remove damaged and inflamed keratinocyte cells. New immature DCs are also recruited by CCL20 via chemotaxis where their activation restarts and amplifies the cycle of inflammation. IL-17 and additional cytokines released from the influx of neutrophils, T and dendritic cells mediate effects on localized leukocytes and keratinocytes that supports the progression of psoriasis by inciting chronic inflammation.
Role in asthma
The IL-17F gene was discovered in 2001, and is located on chromosome 6p12. Notably, among this family, IL-17F has been well characterized both in vitro and in vivo, and has been shown to have a pro-inflammatory role in asthma. IL-17F is clearly expressed in the airway of asthmatics and its expression level is correlated with disease severity. Moreover, a coding region variant (H161R) of the IL-17F gene is inversely associated with asthma and encodes an antagonist for the wild-type IL-17F. IL-17F is able to induce several cytokines, chemokines and adhesion molecules in bronchial epithelial cells, vein endothelial cells, fibroblasts and eosinophils. IL-17F utilizes IL-17RA and IL-17RC as its receptors, and activates the MAP kinase related pathway. IL-17F is derived from several cell types such as Th17 cells, mast cells and basophils, and shows a wide tissue expression pattern including lung. Overexpression of IL-17F gene in the airway of mice is associated with airway neutrophilia, the induction of many cytokines, an increase in airway hyperreactivity, and mucus hypersecretion. Hence, IL-17F may have a crucial role in allergic airway inflammation, and have important therapeutic implications in asthma.
Therapeutic target
Because of its involvement in immune regulatory functions, IL-17 inhibitors are being investigated as possible treatments for autoimmune diseases such as rheumatoid arthritis, psoriasis and inflammatory bowel disease. In January 2015, the FDA approved the use of secukinumab (trade name Cosentyx), an IL-17 inhibiting monoclonal antibody, for the treatment of moderate to severe plaque psoriasis. In addition, Cosentyx has been approved in Japan for use in treating psoriatic arthritis. The anti-IL-23 antibody ustekinumab can also be used to effectively treat psoriasis by reducing IL-17.
Based on emerging evidence from animal models, IL-17 has been suggested as a target for anti-inflammatory therapies to improve recovery post-stroke and to reduce the formation of skin cancer. IL-17 has also been implicated in multiple sclerosis.
Receptors
The IL-17 receptor family consists of five, broadly distributed receptors (IL-17RA, B, C, D and E) that present with individual ligand specificities. Within this family of receptors, IL-17RA is the best-described. IL-17RA binds both IL-17A and IL-17F and is expressed in multiple tissues: vascular endothelial cells, peripheral T cells, B cell lineages, fibroblast, lung, myelomonocytic cells, and marrow stromal cells. Signal transduction for both IL-17A and IL-17F requires the presence of a heterodimeric complex consisting of both IL-17RA and IL-17RC and the absence of either receptor results in ineffective signal transduction. This pattern is reciprocated for other members of the IL-17 family such as IL-17E, which requires an IL-17RA-IL-17RB complex (also known as IL-17Rh1, IL-17BR or IL-25R) for effective function.
Another member of this receptor family, IL-17RB, binds both IL-17B and IL-17E. Furthermore, it is expressed in the kidney, pancreas, liver, brain, and intestine. IL-17RC is expressed by the prostate, cartilage, kidney, liver, heart, and muscle, and its gene may undergo alternate splicing to produce a soluble receptor in addition to its cell membrane-bound form. In similar manner, the gene for IL-17RD may undergo alternative splicing to yield a soluble receptor. This feature may allow these receptors to inhibit the stimulatory effects of their yet-undefined ligands. The least-described of these receptors, IL-17RE, is known to be expressed in the pancreas, brain, and prostate.
Signal transduction by these receptors is as diverse as their distribution. These receptors do not exhibit a significant similarity in extracellular or intracellular amino acid sequence when compared to other cytokine receptors. Transcription factors such as TRAF6, JNK, Erk1/2, p38, AP-1 and NF-κB have been implicated in IL-17 mediated signaling in a stimulation-dependent, tissue-specific manner. Other signaling mechanisms have also been proposed, but more work is needed to fully elucidate the true signaling pathways used by these diverse receptors.