
Pronunciation /oʊˈmɛprəzoʊl/ License data US FDA: Omeprazole Molar mass 345.42 g/mol Protein binding 95% | AHFS/Drugs.com Monograph Routes ofadministration by mouth, IV CAS ID 73590-58-6 | |
 | ||
Trade names Losec, Prilosec, Zegerid, others Pregnancycategory AU: B3US: C (Risk not ruled out) | ||
Omeprazole, sold under the brand names Prilosec and Losec among others, is a medication used in the treatment of gastroesophageal reflux disease, peptic ulcer disease, and Zollinger–Ellison syndrome. It is also used to prevent upper gastrointestinal bleeding in people who are at high risk. It can be taken by mouth or injected into a vein.
Contents
- Side effects of nexium omeprazole and protonix on the kidneys
- Medical uses
- Peptic ulcers
- Adverse effects
- Pregnancy and breast feeding
- Interactions
- Mechanism of action
- Pharmacokinetics
- Chemistry
- Measurement in body fluids
- History
- Dosage forms
- References
Common side effects include nausea, vomiting, headaches, and increased intestinal gas. Serious side effects may include Clostridium difficile colitis, an increased risk of pneumonia, an increased risk of bone fractures, and the potential of masking stomach cancer. It is unclear if it is safe for use in pregnancy. Omeprazole is a proton pump inhibitor and as such blocks the release of stomach acid.
Omeprazole was discovered in 1979. It is on the World Health Organization's List of Essential Medicines, the most effective and safe medicines needed in a health system. It is available as a generic medication. The wholesale cost in the developing world as of 2014 is US$0.01 to US$0.07 per dose. In the United States it costs on average US$0.50 per pill.
Side effects of nexium omeprazole and protonix on the kidneys
Medical uses
Omeprazole can be used in the treatment of gastroesophageal reflux disease (GERD), peptic ulcers, erosive esophagitis, and Zollinger-Ellison syndrome.
Peptic ulcers
Peptic ulcers may be treated with omeprazole. Treatment of H. pylori infection can be completed by taking a triple therapy combination of omeprazole, amoxicillin, and clarithromycin for 7–14 days. Amoxicillin may be replaced with metronidazole in patients who are allergic to penicillin.
Adverse effects
The most frequent significant adverse effects occurring in at least 1% of patients include:
Other significant concerns related to adverse effects are:
Concern has been expressed regarding vitamin B12 and iron malabsorption, but effects seem to be clinically insignificant, especially when supplement therapy is provided.
Since their introduction, proton pump inhibitors (PPIs, especially omeprazole) have also been associated with several cases of acute interstitial nephritis, an inflammation of the kidneys that often occurs as an adverse drug reaction.
Long-term use of PPIs is strongly associated with the development of benign polyps from fundic glands (which is distinct from fundic gland polyposis); these polyps do not cause cancer and resolve when PPIs are discontinued. No association is seen between PPI use and cancer, but use of PPIs may mask gastric cancers or other serious gastric problems and physicians should be aware of this effect.
Pregnancy and breast-feeding
Epidemiological data do not show an increased risk of major birth defects after maternal use of omeprazole during pregnancy.
No clinical trials have deeply evaluated the potential consequences of the use of omeprazole in breastfeeding. However, the pharmacokinetics of omeprazole molecule strongly suggest the safety of omeprazole use during breastfeeding:
Omeprazole at normal doses is likely safe during breastfeeding.
Interactions
Important drug interactions are rare.
However, the most significant major drug interaction concern is the decreased activation of clopidogrel when taken together with omeprazole. Although still controversial, this may increase the risk of stroke or heart attack in people taking clopidogrel to prevent these events.
This interaction is possible because omeprazole is an inhibitor of the enzymes CYP2C19 and CYP3A4. Clopidogrel is an inactive prodrug that partially depends on CYP2C19 for conversion to its active form. Inhibition of CYP2C19 may block the activation of clopidogrel, which could reduce its effects.
Almost all benzodiazepines are metabolised by the CYP3A4 and CYP2D6 pathway, and inhibition of these enzymes results in a higher AUC (i.e. the total effect over time of a given dose). Other examples of drugs dependent on CYP3A4 for their metabolism are escitalopram, warfarin, oxycodone, tramadol, and oxymorphone. The concentrations of these drugs may increase if they are used concomitantly with omeprazole.
Omeprazole is also a competitive inhibitor of p-glycoprotein, as are other PPIs.
Drugs that depend on an acidic stomach environment (such as ketoconazole or atazanavir) may be poorly absorbed, whereas acid-labile antibiotics (such as erythromycin which is a very strong CYP3A4 inhibitor) may be absorbed to a greater extent than normal due to the more alkaline environment of the stomach.
St. John's wort (Hypericum perforatum) and Gingko biloba significantly reduce plasma concentrations of omeprazole through induction of CYP3A4 and CYP2C19.
Proton-pump inhibitors like omeprazole have been found to increase the plasma concentrations of methotrexate.
Mechanism of action
Omeprazole is a selective and irreversible proton pump inhibitor. It suppresses stomach acid secretion by specific inhibition of the H+/K+-ATPase system found at the secretory surface of gastric parietal cells. Because this enzyme system is regarded as the acid (proton, or H+) pump within the gastric mucosa, omeprazole inhibits the final step of acid production.
Omeprazole also inhibits both basal and stimulated acid secretion irrespective of the stimulus.
The inhibitory effect of omeprazole occurs within 1 hour after oral administration. The maximum effect occurs within 2 hours. The duration of inhibition is up to 72 hours. When omeprazole is stopped, baseline stomach acid secretory activity returns after 3 to 5 days. The inhibitory effect of omeprazole on acid secretion will plateau after 4 days of repeated daily dosing.
Pharmacokinetics
The absorption of omeprazole takes place in the small intestine and is usually completed within 3 to 6 hours. The systemic bioavailability of omeprazole after repeated dose is about 60%.
Omeprazole, as well as other PPIs, are only effective on active H+/K+-ATPase pumps. These pumps are stimulated in the presence of food to aid in digestion. For this reason, patients should be advised to take omeprazole with a glass of water on an empty stomach. Additionally, most sources recommend that after taking omeprazole, at least 30 minutes should be allowed to elapse before eating (at least 60 minutes for immediate-release omeprazole plus sodium bicarbonate products, such as Zegerid), though some sources say that with delayed-release forms of omeprazole, waiting before eating after taking the medication is not necessary.
Omeprazole is completely metabolized by the cytochrome P450 system, mainly in the liver. Identified metabolites are the sulfone, the sulfide, and hydroxy-omeprazole, which exert no significant effect on acid secretion. About 80% of an orally given dose is excreted as metabolites in the urine, and the remainder is found in the feces, primarily originating from bile secretion.
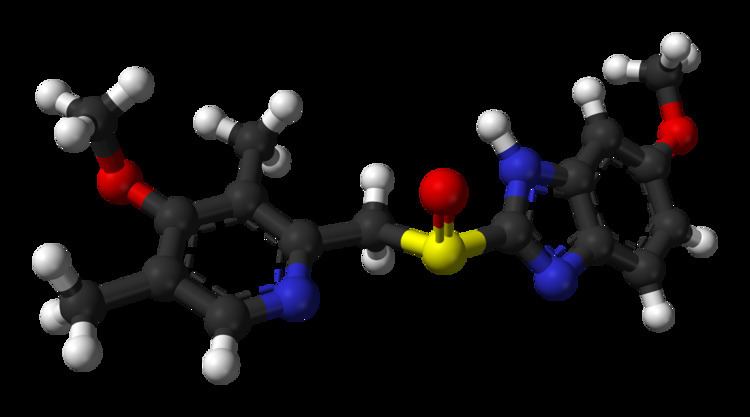
Chemistry
Omeprazole contains a tricoordinated sulfinyl sulfur in a pyramidal structure and therefore can exist as either the (S)- or (R)-enantiomers. Omeprazole is a racemate, an equal mixture of the two. In the acidic conditions of the canaliculi of parietal cells, both enantiomers are converted to chiral products (sulfenic acid and sulfenamide configurations) which react with a cysteine group in H+/K+ ATPase, thereby inhibiting the ability of the parietal cells to produce gastric acid.
AstraZeneca has also developed esomeprazole (Nexium) which is a eutomer, purely the (S)-enantiomer, rather than a racemate like omeprazole.
Omeprazole undergoes a chiral shift in vivo which converts the inactive (R)-enantiomer to the active (S)-enantiomer, doubling the concentration of the active form. This chiral shift is accomplished by the CYP2C19 isozyme of cytochrome P450, which is not found equally in all human populations. Those who do not metabolize the drug effectively are called "poor metabolizers". The proportion of the poor metabolizer phenotype varies widely between populations, from 2.0–2.5% in African Americans and white Americans to >20% in Asians; several pharmacogenomics studies have suggested that PPI treatment should be tailored according to CYP2C19 metabolism status.
Measurement in body fluids
Omeprazole may be quantified in plasma or serum to monitor therapy or to confirm a diagnosis of poisoning in hospitalized patients. Plasma omeprazole concentrations are usually in a range of 0.2–1.2 mg/l in persons receiving the drug therapeutically by the oral route and 1–6 mg/l in victims of acute overdose. Enantiomeric chromatographic methods are available to distinguish esomeprazole from racemic omeprazole.
History
Omeprazole was first marketed in the United States in 1989 by Astra AB, now AstraZeneca, under the brand name Losec. In 1990, at the request of the U.S. Food and Drug Administration, the brand name Losec was changed to Prilosec to avoid confusion with the diuretic Lasix (furosemide). The new name led to confusion between omeprazole (Prilosec) and fluoxetine (Prozac), an antidepressant.
When Prilosec's U.S. patent expired in April 2001, AstraZeneca introduced esomeprazole (Nexium) as a patented replacement drug. Many companies introduced generics as AstraZeneca's patents expired worldwide, which are available under many brand names.
Dosage forms
Omeprazole is available as tablets and capsules (containing omeprazole or omeprazole magnesium) in strengths of 10, 20, 40, and in some markets 80 mg; and as a powder (omeprazole sodium) for intravenous injection. Most oral omeprazole preparations are enteric-coated, due to the rapid degradation of the drug in the acidic conditions of the stomach. This is most commonly achieved by formulating enteric-coated granules within capsules, enteric-coated tablets, and the multiple-unit pellet system (MUPS). An immediate release formulation was approved by the FDA in the United States, which does not require enteric coating.
It is also available for use in injectable form (IV) in Europe, but not in the U.S. The injection pack is a combination pack consisting of a vial and a separate ampule of reconstituting solution. Each 10-ml clear glass vial contains a white to off-white lyophilised powder consisting of omeprazole sodium 42.6 mg, equivalent to 40 mg of omeprazole.
Omeprazole is also available as an oral suspension of enteric-coated beads in the UK as an unlicensed product. Oral suspensions are predominantly used for children, but can also be used by those with difficulty swallowing or those using a feeding tube.