
ICD-10-PCS [1] | MeSH D005307 | |
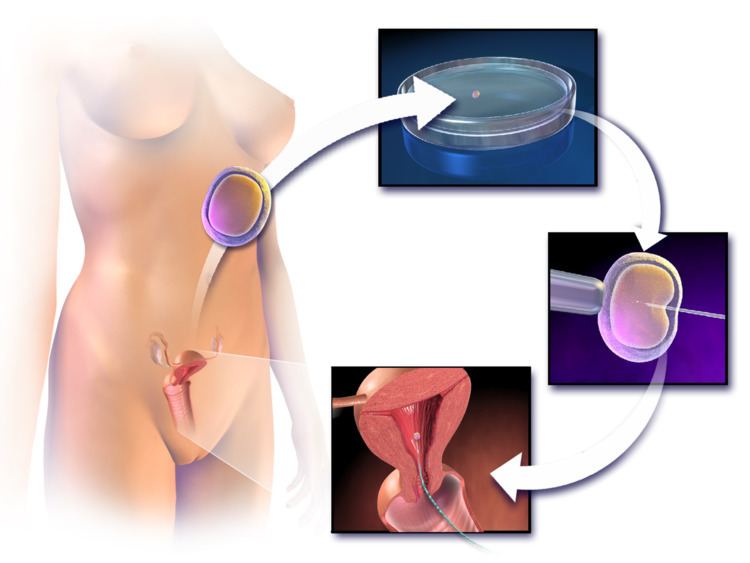 | ||
In vitro fertilisation (or fertilization; IVF) is a process by which an egg is fertilised by sperm outside the body: in vitro ("in glass"). The process involves monitoring and stimulating a woman's ovulatory process, removing an ovum or ova (egg or eggs) from the woman's ovaries and letting sperm fertilise them in a liquid in a laboratory. The fertilised egg (zygote) is cultured for 2–6 days in a growth medium and is then transferred to the same or another woman's uterus, with the intention of establishing a successful pregnancy.
Contents
- Terminology
- Medical uses
- Success rates
- Live birth rate
- Pregnancy rate
- Predictors of success
- Multiple births
- Spread of infectious disease
- Other risks to the egg providerretriever
- Birth defects
- Other risks to the offspring
- Method
- Ovarian hyperstimulation
- Natural IVF
- Final maturation induction
- Egg retrieval
- Egg and sperm preparation
- Co incubation
- Embryo culture
- Embryo selection
- Embryo transfer
- Adjunctive medication
- Expansions
- Preimplantation genetic screening or diagnosis
- Cryopreservation
- Other expansions
- Leftover embryos or eggs
- History
- Mix ups
- Preimplantation genetic diagnosis or screening
- Autonomy and Tissue Ownership
- Profit desire of the industry
- Pregnancy past menopause
- Same sex couples single and unmarried parents
- Anonymous donors
- Unwanted embryos
- Religious response
- Society and culture
- Emotional involvement
- Men and IVF
- Availability and utilisation
- USA
- Australia
- Cameroon
- Israel
- United Kingdom
- Legal status
- References
IVF is a type of assisted reproductive technology used for infertility treatment and gestational surrogacy, in which a fertilized egg is implanted into a surrogate's uterus, and the resulting child is genetically unrelated to the surrogate. Some countries banned or otherwise regulate the availability of IVF treatment, giving rise to fertility tourism. Restrictions on availability of IVF include costs and age to carry a healthy pregnancy to term. IVF is mostly attempted if less invasive or expensive options have failed or are unlikely to work.
The first successful birth of a "test tube baby", Louise Brown, occurred in 1978. Louise Brown was born as a result of natural cycle IVF where no stimulation was made. Robert G. Edwards was awarded the Nobel Prize in Physiology or Medicine in 2010, the physiologist who co-developed the treatment together with Patrick Steptoe; Steptoe was not eligible for consideration as the Nobel Prize is not awarded posthumously. With egg donation and IVF, women who are past their reproductive years or have reached menopause can still become pregnant. Adriana Iliescu held the record as the oldest woman to give birth using IVF and donated egg, when she gave birth in 2004 at the age of 66, a record passed in 2006. After the IVF treatment many couples are able to get pregnant without any fertility treatments. In 2012 it was estimated that five million children had been born worldwide using IVF and other assisted reproduction techniques.
Terminology
The term in vitro, from the Latin meaning in glass, is used, because early biological experiments involving cultivation of tissues outside the living organism from which they came, were carried out in glass containers such as beakers, test tubes, or petri dishes.
Today, the scientific term in vitro is used to refer to any biological procedure that is performed outside the organism in which it would normally have occurred, to distinguish it from an in vivo procedure, where the tissue remains inside the living organism within which it is normally found. A colloquial term for babies conceived as the result of IVF, "test tube babies", refers to the tube-shaped containers of glass or plastic resin, called test tubes, that are commonly used in chemistry labs and biology labs. However, in vitro fertilisation is usually performed in the shallower containers called Petri dishes. One IVF method, autologous endometrial coculture, is actually performed on organic material, but is still considered in vitro.
Medical uses
IVF may be used to overcome female infertility where it is due to problems with the fallopian tubes, making fertilisation in vivo difficult. It can also assist in male infertility, in those cases where there is a defect in sperm quality; in such situations intracytoplasmic sperm injection (ICSI) may be used, where a sperm cell is injected directly into the egg cell. This is used when sperm has difficulty penetrating the egg, and in these cases the partner's or a donor's sperm may be used. ICSI is also used when sperm numbers are very low. When indicated, the use of ICSI has been found to increase the success rates of IVF.
According to the British NICE guidelines, IVF treatment is appropriate in cases of unexplained infertility for women that have not conceived after 2 years of regular unprotected sexual intercourse. This rule does not apply to all countries. (See infertility.)
IVF is also considered suitable in cases where any of its expansions is of interest, that is, a procedure that is usually not necessary for the IVF procedure itself, but would be virtually impossible or technically difficult to perform without concomitantly performing methods of IVF. Such expansions include preimplantation genetic diagnosis (PGD) to rule out presence of genetic disorders, as well as egg donation or surrogacy where the woman providing the egg isn't the same who will carry the pregnancy to term. Further details in the Expansions-section below.
Success rates
IVF success rates, the percentage of all IVF procedures which result in a favourable outcome. Depending on the type of calculation used, this outcome may represent the number of confirmed pregnancies, called the pregnancy rate, or the number of live births, called the live birth rate. The success rate depends on variable factors such as maternal age, cause of infertility, embryo status, reproductive history and lifestyle factors.
Maternal age: Younger candidates of IVF are more likely to get pregnant. Women older than 41 are more likely to get pregnant with a donor egg.
Reproductive history: Women who have been previously pregnant are in many cases more successful with IVF treatments than those who have never been pregnant.
Due to advances in reproductive technology, IVF success rates are substantially higher today than they were just a few years ago.
Live birth rate
The live birth rate is the percentage of all IVF cycles that lead to a live birth. This rate does not include miscarriage or stillbirth and multiple-order births such as twins and triplets are counted as one pregnancy. A 2012 summary compiled by the Society for Reproductive Medicine which reports the average IVF success rates in the United States per age group using non-donor eggs compiled the following data:
In 2006, Canadian clinics reported a live birth rate of 27%. Birth rates in younger patients were slightly higher, with a success rate of 35.3% for those 21 and younger, the youngest group evaluated. Success rates for older patients were also lower and decrease with age, with 37-year-olds at 27.4% and no live births for those older than 48, the oldest group evaluated. Some clinics exceeded these rates, but it is impossible to determine if that is due to superior technique or patient selection, because it is possible to artificially increase success rates by refusing to accept the most difficult patients or by steering them into oocyte donation cycles (which are compiled separately). Further, pregnancy rates can be increased by the placement of several embryos at the risk of increasing the chance for multiples.
The live birth rates using donor eggs are also given by the SART and include all age groups using either fresh or thawed eggs.
Because not each IVF cycle that is started will lead to oocyte retrieval or embryo transfer, reports of live birth rates need to specify the denominator, namely IVF cycles started, IVF retrievals, or embryo transfers. The Society for Assisted Reproductive Technology (SART) summarised 2008-9 success rates for US clinics for fresh embryo cycles that did not involve donor eggs and gave live birth rates by the age of the prospective mother, with a peak at 41.3% per cycle started and 47.3% per embryo transfer for patients under 35 years of age.
IVF attempts in multiple cycles result in increased cumulative live birth rates. Depending on the demographic group, one study reported 45% to 53% for three attempts, and 51% to 71% to 80% for six attempts.
Pregnancy rate
Pregnancy rate may be defined in various ways. In the United States, the pregnancy rate used by the Society for Assisted Reproductive Technology and the Centers for Disease Control (and appearing in the table in the Success Rates section above) are based on fetal heart motion observed in ultrasound examinations.
The 2009 summary compiled by the Society for Reproductive Medicine included the following data for the United States:
In 2006, Canadian clinics reported an average pregnancy rate of 35%. A French study estimated that 66% of patients starting IVF treatment finally succeed in having a child (40% during the IVF treatment at the centre and 26% after IVF discontinuation). Achievement of having a child after IVF discontinuation was mainly due to adoption (46%) or spontaneous pregnancy (42%).
Predictors of success
The main potential factors that influence pregnancy (and live birth) rates in IVF have been suggested to be maternal age, duration of infertility or subfertility, bFSH and number of oocytes, all reflecting ovarian function. Optimal woman’s age is 23–39 years at time of treatment.
Biomarkers that affect the pregnancy chances of IVF include:
Other determinants of outcome of IVF include:
Aspirin is sometimes prescribed to women for the purpose of increasing the chances of conception by IVF, but there is insufficient evidence to show that it actually works.
A 2013 review and metaanalysis of randomised controlled trials of acupuncture as an adjuvant therapy in IVF found no overall benefit, and concluded that an apparent benefit detected in a subset of published trials where the control group (those not using acupuncture) experienced a lower than average rate of pregnancy requires further study, due to the possibility of publication bias and other factors.
A Cochrane review came to the result that endometrial injury performed in the month prior to ovarian induction appeared to increase both the live birth rate and clinical pregnancy rate in IVF compared with no endometrial injury. There was no evidence of a difference between the groups in miscarriage, multiple pregnancy or bleeding rates. Evidence suggested that endometrial injury on the day of oocyte retrieval was associated with a lower live birth or ongoing pregnancy rate.
For women, intake of antioxidants (such as N-acetyl-cysteine, melatonin, vitamin A, vitamin C, vitamin E, folic acid, myo-inositol, zinc or selenium) has not been associated with a significantly increased live birth rate or clinical pregnancy rate in IVF according to Cochrane reviews. The review found that oral antioxidants given to men in couples with male factor or unexplained subfertility may improve live birth rates, but more evidence is needed.
A Cochrane review in 2015 came to the result that there is no evidence identified regarding the effect of pre-conception lifestyle advice on the chance of a live birth outcome.
Multiple births
The major complication of IVF is the risk of multiple births. This is directly related to the practice of transferring multiple embryos at embryo transfer. Multiple births are related to increased risk of pregnancy loss, obstetrical complications, prematurity, and neonatal morbidity with the potential for long term damage. Strict limits on the number of embryos that may be transferred have been enacted in some countries (e.g. Britain, Belgium) to reduce the risk of high-order multiples (triplets or more), but are not universally followed or accepted. Spontaneous splitting of embryos in the womb after transfer can occur, but this is rare and would lead to identical twins. A double blind, randomised study followed IVF pregnancies that resulted in 73 infants (33 boys and 40 girls) and reported that 8.7% of singleton infants and 54.2% of twins had a birth weight of < 2,500 grams (5.5 lb).
Recent evidence also suggest that singleton offspring after IVF is at higher risk for lower birth weight for unknown reasons.
Spread of infectious disease
By sperm washing, the risk that a chronic disease in the male providing the sperm would infect the female or offspring can be brought to negligible levels.
In males with hepatitis B, The Practice Committee of the American Society for Reproductive Medicine advises that sperm washing is not necessary in IVF to prevent transmission, unless the female partner has not been effectively vaccinated. In females with hepatitis B, the risk of vertical transmission during IVF is no different from the risk in spontaneous conception. However, there is not enough evidence to say that ICSI procedures are safe in females with hepatitis B in regard to vertical transmission to the offspring.
Regarding potential spread of HIV/AIDS, Japan's government prohibited the use of in vitro fertilisation procedures for couples in which both partners are infected with HIV. Despite the fact that the ethics committees previously allowed the Ogikubo, Tokyo Hospital, located in Tokyo, to use in vitro fertilisation for couples with HIV, the Ministry of Health, Labour and Welfare of Japan decided to block the practice. Hideji Hanabusa, the vice president of the Ogikubo Hospital, states that together with his colleagues, he managed to develop a method through which scientists are able to remove HIV from sperm.
Other risks to the egg provider/retriever
A risk of ovarian stimulation is the development of ovarian hyperstimulation syndrome, particularly if hCG is used for inducing final oocyte maturation. This results in swollen, painful ovaries. It occurs in 30% of patients. Mild cases can be treated with over the counter medications and cases can be resolved in the absence of pregnancy. In moderate cases, ovaries swell and fluid accumulated in the abdominal cavities and may have symptoms of heartburn, gas, nausea or loss of appetite. In severe cases patients have sudden excess abdominal pain, nausea, vomiting and will result in hospitalisation.
During egg retrieval, there’s a small chance of bleeding, infection, and damage to surrounding structures like bowel and bladder (transvaginal ultrasound aspiration) as well as difficulty in breathing, chest infection, allergic reactions to medication, or nerve damage (laproscopy).
Ectopic pregnancy may also occur if a fertilised egg develops outside the uterus, usually in the fallopian tubes and requires immediate destruction of the fetus.
IVF does not seem to be associated with an elevated risk of cervical cancer, nor with ovarian cancer or endometrial cancer when neutralising the confounder of infertility itself. Nor does it seem to impart any increased risk for breast cancer.
Regardless of pregnancy result, IVF treatment is usually stressful for patients. Neuroticism and the use of escapist coping strategies are associated with a higher degree of distress, while the presence social support has a relieving effect. A negative pregnancy test after IVF is associated with an increased risk for depression in women, but not with any increased risk of developing anxiety disorders. Pregnancy test results do not seem to be a risk factor for depression or anxiety among men.
Birth defects
A review in 2013 came to the result that infants resulting from IVF (with or without ICSI) have a relative risk of birth defects of 1.32 (95% confidence interval 1.24–1.42) compared to naturally conceived infants. In 2008, an analysis of the data of the National Birth Defects Study in the US found that certain birth defects were significantly more common in infants conceived through IVF, notably septal heart defects, cleft lip with or without cleft palate, esophageal atresia, and anorectal atresia; the mechanism of causality is unclear. However, in a population-wide cohort study of 308,974 births (with 6163 using assisted reproductive technology and following children from birth to age five) researchers found: "The increased risk of birth defects associated with IVF was no longer significant after adjustment for parental factors." Parental factors included known independent risks for birth defects such as maternal age, smoking status, etc. Multivariate correction did not remove the significance of the association of birth defects and ICSI (corrected odds ratio 1.57), although the authors speculate that underlying male infertility factors (which would be associated with the use of ICSI) may contribute to this observation and were not able to correct for these confounders. The authors also found that a history of infertility elevated risk itself in the absence of any treatment (odds ratio 1.29), consistent with a Danish national registry study and "...implicates patient factors in this increased risk." The authors of the Danish national registry study speculate: "...our results suggest that the reported increased prevalence of congenital malformations seen in singletons born after assisted reproductive technology is partly due to the underlying infertility or its determinants."
Other risks to the offspring
If the underlying infertility is related to abnormalities in spermatogenesis, it is plausible, but too early to examine that male offspring are at higher risk for sperm abnormalities.
IVF does not seem to confer any risks regarding cognitive development, school performance, social functioning and behaviour. Also, IVF infants are known to be as securely attached to their parents as those who were naturally conceived, and IVF adolescents are as well-adjusted as those who have been naturally conceived.
Limited long-term follow-up data suggest that IVF may be associated with an increased incidence of hypertension, impaired fasting glucose, increase in total body fat composition, advancement of bone age, subclinical thyroid disorder, early adulthood clinical depression and binge drinking in the offspring. It is not known, however, whether these potential associations are caused by the IVF procedure in itself, by adverse obstetric outcomes associated with IVF, by the genetic origin of the children or by yet unknown IVF-associated causes. Increases in embryo manipulation during IVF result in more deviant fetal growth curves, but birth weight does not seem to be a reliable marker of fetal stress.
IVF, including ICSI, is associated with an increased risk of imprinting disorders (including Prader-Willi syndrome and Angelman syndrome), with an odds ratio of 3.7 (95% confidence interval 1.4 to 9.7).
An IVF-associated incidence of cerebral palsy and neurodevelopmental delay are believed to be related to the confounders of prematurity and low birthweight. Similarly, an IVF-associated incidence of autism and attention-deficit disorder are believed to be related to confounders of maternal and obstetric factors.
Overall, IVF does not cause an increased risk of childhood cancer. Studies have shown a decrease in the risk of certain cancers and an increased risks of certain others including retinoblastoma hepatoblastoma and rhabdomyosarcoma.
Method
Theoretically, in vitro fertilisation could be performed by collecting the contents from a woman's fallopian tubes or uterus after natural ovulation, mixing it with sperm, and reinserting the fertilised ova into the uterus. However, without additional techniques, the chances of pregnancy would be extremely small. The additional techniques that are routinely used in IVF include ovarian hyperstimulation to generate multiple eggs or ultrasound-guided transvaginal oocyte retrieval directly from the ovaries; after which the ova and sperm are prepared, as well as culture and selection of resultant embryos before embryo transfer into a uterus.
Ovarian hyperstimulation
Ovarian hyperstimulation is the stimulation to induce development of multiple follicles of the ovaries. It should start with response prediction by e.g. age, antral follicle count and level of anti-Müllerian hormone. The resulting prediction of e.g. poor or hyper-response to ovarian hyperstimulation determines the protocol and dosage for ovarian hyperstimulation.
Ovarian hyperstimulation also includes suppression of spontaneous ovulation, for which two main methods are available: Using a (usually longer) GnRH agonist protocol or a (usually shorter) GnRH antagonist protocol. In a standard long GnRH agonist protocol the day when hyperstimulation treatment is started and the expected day of later oocyte retrieval can be chosen to conform to personal choice, while in a GnRH antagonist protocol it must be adapted to the spontaneous onset of the previous menstruation. On the other hand, the GnRH antagonist protocol has a lower risk of ovarian hyperstimulation syndrome (OHSS), which is a life-threatening complication.
For the ovarian hyperstimulation in itself, injectable gonadotropins (usually FSH analogues) are generally used under close monitoring. Such monitoring frequently checks the estradiol level and, by means of gynecologic ultrasonography, follicular growth. Typically approximately 10 days of injections will be necessary.
Natural IVF
There are several methods termed natural cycle IVF:
IVF using no drugs for ovarian hyperstimulation was the method for the conception of Louise Brown. This method can be successfully used when women want to avoid taking ovarian stimulating drugs with its associated side-effects. HFEA has estimated the live birth rate to be approximately 1.3% per IVF cycle using no hyperstimulation drugs for women aged between 40–42.
Mild IVF is a method where a small dose of ovarian stimulating drugs are used for a short duration during a woman’s natural cycle aimed at producing 2–7 eggs and creating healthy embryos. This method appears to be an advance in the field to reduce complications and side-effects for women and it is aimed at quality, and not quantity of eggs and embryos. One study comparing a mild treatment (mild ovarian stimulation with GnRH antagonist co-treatment combined with single embryo transfer) to a standard treatment (stimulation with a GnRH agonist long-protocol and transfer of two embryos) came to the result that the proportions of cumulative pregnancies that resulted in term live birth after 1 year were 43.4% with mild treatment and 44.7% with standard treatment. Mild IVF can be cheaper than conventional IVF and with a significantly reduced risk of multiple gestation and OHSS.
Final maturation induction
When the ovarian follicles have reached a certain degree of development, induction of final oocyte maturation is performed, generally by an injection of human chorionic gonadotropin (hCG). Commonly, this is known as the "trigger shot." hCG acts as an analogue of luteinising hormone, and ovulation would occur between 38 and 40 hours after a single HCG injection, but the egg retrieval is performed at a time usually between 34 and 36 hours after hCG injection, that is, just prior to when the follicles would rupture. This avails for scheduling the egg retrieval procedure at a time where the eggs are fully mature. HCG injection confers a risk of ovarian hyperstimulation syndrome. Using a GnRH agonist instead of hCG eliminates the risk of ovarian hyperstimulation syndrome, but with a delivery rate of approximately 6% less than with hCG.
Egg retrieval
The eggs are retrieved from the patient using a transvaginal technique called transvaginal oocyte retrieval, involving an ultrasound-guided needle piercing the vaginal wall to reach the ovaries. Through this needle follicles can be aspirated, and the follicular fluid is passed to an embryologist to identify ova. It is common to remove between ten and thirty eggs. The retrieval procedure usually takes between 20 and 40 minutes, depending on the number of mature follicles, and is usually done under conscious sedation or general anaesthesia.
Egg and sperm preparation
In the laboratory, the identified eggs are stripped of surrounding cells and prepared for fertilisation. An oocyte selection may be performed prior to fertilisation to select eggs with optimal chances of successful pregnancy. In the meantime, semen is prepared for fertilisation by removing inactive cells and seminal fluid in a process called sperm washing. If semen is being provided by a sperm donor, it will usually have been prepared for treatment before being frozen and quarantined, and it will be thawed ready for use.
Co-incubation
The sperm and the egg are incubated together at a ratio of about 75,000:1 in a culture media in order for the actual fertilisation to take place. A review in 2013 came to the result that a duration of this co-incubation of about 1 to 4 hours results in significantly higher pregnancy rates than 16 to 24 hours. In most cases, the egg will be fertilised during co-incubation and will show two pronuclei. In certain situations, such as low sperm count or motility, a single sperm may be injected directly into the egg using intracytoplasmic sperm injection (ICSI). The fertilised egg is passed to a special growth medium and left for about 48 hours until the egg consists of six to eight cells.
In gamete intrafallopian transfer, eggs are removed from the woman and placed in one of the fallopian tubes, along with the man's sperm. This allows fertilisation to take place inside the woman's body. Therefore, this variation is actually an in vivo fertilisation, not an in vitro fertilisation.
Embryo culture
The main durations of embryo culture are until cleavage stage (day two to four after co-incubation) or the blastocyst stage (day five or six after co-incubation). Embryo culture until the blastocyst stage confers a significant increase in live birth rate per embryo transfer, but also confers a decreased number of embryos available for transfer and embryo cryopreservation, so the cumulative clinical pregnancy rates are increased with cleavage stage transfer. Transfer day two instead of day three after fertilisation has no differences in live birth rate. There are significantly higher odds of preterm birth (odds ratio 1.3) and congenital anomalies (odds ratio 1.3) among births having from embryos cultured until the blastocyst stage compared with cleavage stage.
Embryo selection
Laboratories have developed grading methods to judge oocyte and embryo quality. In order to optimise pregnancy rates, there is significant evidence that a morphological scoring system is the best strategy for the selection of embryos. Since 2009 where the first time-lapse microscopy system for IVF was approved for clinical use, morphokinetic scoring systems has shown to improve to pregnancy rates further. However, when all different types of time-lapse embryo imaging devices, with or without morphokinetic scoring systems, are compared against conventional embryo assessment for IVF, there is insufficient evidence of a difference in live-birth, pregnancy, stillbirth or miscarriage to choose between them.
Embryo transfer
Embryos are graded by the embryologist based on the amount of cells, evenness of growth and degree of fragmentation. The number to be transferred depends on the number available, the age of the woman and other health and diagnostic factors. In countries such as Canada, the UK, Australia and New Zealand, a maximum of two embryos are transferred except in unusual circumstances. In the UK and according to HFEA regulations, a woman over 40 may have up to three embryos transferred, whereas in the USA, younger women may have many embryos transferred based on individual fertility diagnosis. Most clinics and country regulatory bodies seek to minimise the risk of pregnancies carrying multiples, as it is not uncommon for more implantations to take than desired. The embryos judged to be the "best" are transferred to the patient's uterus through a thin, plastic catheter, which goes through her vagina and cervix. Several embryos may be passed into the uterus to improve chances of implantation and pregnancy.
Adjunctive medication
Luteal support is the administration of medication, generally progesterone, progestins or GnRH agonists, to increase the success rate of implantation and early embryogenesis, thereby complementing and/or supporting the function of the corpus luteum. A Cochrane review found that hCG or progesterone given during the luteal phase may be associated with higher rates of live birth or ongoing pregnancy, but that the evidence is not conclusive. Co-treatment with GnRH agonists appears to improve outcomes, by a live birth rate RD of +16% (95% confidence interval +10 to +22%).
On the other hand, growth hormone or aspirin as adjunctive medication in IVF have no evidence of overall benefit.
Expansions
There are various expansions or additional techniques that can be applied in IVF, which are usually not necessary for the IVF procedure itself, but would be virtually impossible or technically difficult to perform without concomitantly performing methods of IVF.
Preimplantation genetic screening or diagnosis
Preimplantation genetic screening (PGS) or preimplantation genetic diagnosis (PGD) has been suggested to be able to be used in IVF to select an embryo that appears to have the greatest chances for successful pregnancy. However, a systematic review and meta-analysis of existing randomised controlled trials came to the result that there is no evidence of a beneficial effect of PGS with cleavage-stage biopsy as measured by live birth rate. On the contrary, for women of advanced maternal age, PGS with cleavage-stage biopsy significantly lowers the live birth rate. Technical drawbacks, such as the invasiveness of the biopsy, and non-representative samples because of mosaicism are the major underlying factors for inefficacy of PGS.
Still, as an expansion of IVF, patients who can benefit from PGS/PGD include:
PGS screens for numeral chromosomal abnormalities while PGD diagnosis the specific molecular defect of the inherited disease. In both PGS and PGD, individual cells from a pre-embryo, or preferably trophectoderm cells biopsied from a blastocyst, are analysed during the IVF process. Before the transfer of a pre-embryo back to a woman's uterus, one or two cells are removed from the pre-embryos (8-cell stage), or preferably from a blastocyst. These cells are then evaluated for normality. Typically within one to two days, following completion of the evaluation, only the normal pre-embryos are transferred back to the woman's uterus. Alternatively, a blastocyst can be cryopreserved via vitrification and transferred at a later date to the uterus. In addition, PGS can significantly reduce the risk of multiple pregnancies because fewer embryos, ideally just one, are needed for implantation.
Cryopreservation
Cryopreservation can be performed as oocyte cryopreservation before fertilisation, or as embryo cryopreservation after fertilisation.
The Rand Consulting Group has estimated there to be 400,000 frozen embryos in the United States. The advantage is that patients who fail to conceive may become pregnant using such embryos without having to go through a full IVF cycle. Or, if pregnancy occurred, they could return later for another pregnancy. Spare oocytes or embryos resulting from fertility treatments may be used for oocyte donation or embryo donation to another woman or couple, and embryos may be created, frozen and stored specifically for transfer and donation by using donor eggs and sperm. Also, oocyte cryopreservation can be used for women who are likely to lose their ovarian reserve due to undergoing chemotherapy.
The outcome from using cryopreserved embryos has uniformly been positive with no increase in birth defects or development abnormalities.
Other expansions
Leftover embryos or eggs
There may be leftover embryos or eggs from IVF procedures if the woman for whom they were originally created has successfully carried one or more pregnancies to term. With the woman's or couple's permission, these may be donated to help other women or couples as a means of third party reproduction.
In embryo donation, these extra embryos are given to other couples or women for transfer with the goal of producing a successful pregnancy. The resulting child is considered the child of the woman who carries it and gives birth, and not the child of the donor, the same as occurs with egg donation or sperm donation.
Typically, genetic parents donate the eggs to a fertility clinic or where they are preserved by oocyte cryopreservation or embryo cryopreservation until a carrier is found for them. Typically the process of matching the embryo(s) with the prospective parents is conducted by the agency itself, at which time the clinic transfers ownership of the embryos to the prospective parents.
In the United States, women seeking to be an embryo recipient undergo infectious disease screening required by the U.S. Food and Drug Administration (FDA), and reproductive tests to determine the best placement location and cycle timing before the actual Embryo Transfer occurs. The amount of screening the embryo has already undergone is largely dependent on the genetic parents' own IVF clinic and process. The embryo recipient may elect to have her own embryologist conduct further testing.
Alternatives to donating unused embryos are destroying them (or having them implanted at a time where pregnancy is very unlikely), keeping them frozen indefinitely, or donating them for use in research (which results in their unviability). Individual moral views on disposing leftover embryos may depend on personal views on the beginning of human personhood and definition and/or value of potential future persons and on the value that is given to fundamental research questions. Some people believe donation of leftover embryos for research is a good alternative to discarding the embryos when patients receive proper, honest and clear information about the research project, the procedures and the scientific values.
History
In 1977, Steptoe and Edwards successfully carried out a pioneering conception which resulted in the birth of the world's first baby to be conceived by IVF, Louise Brown on 25 July 1978, in Oldham General Hospital, Greater Manchester, UK.
The second successful birth of a test tube baby occurred in India just 67 days after Louise Brown was born. The girl, named Durga conceived in vitro using the methods of Subhash Mukhopadhyay, a physician and researcher from Kolkata.
Mix-ups
In some cases, laboratory mix-ups (misidentified gametes, transfer of wrong embryos) have occurred, leading to legal action against the IVF provider and complex paternity suits. An example is the case of a woman in California who received the embryo of another couple and was notified of this mistake after the birth of her son. This has led to many authorities and individual clinics implementing procedures to minimise the risk of such mix-ups. The HFEA, for example, requires clinics to use a double witnessing system, the identity of specimens is checked by two people at each point at which specimens are transferred. Alternatively, technological solutions are gaining favour, to reduce the manpower cost of manual double witnessing, and to further reduce risks with uniquely numbered RFID tags which can be identified by readers connected to a computer. The computer tracks specimens throughout the process and alerts the embryologist if non-matching specimens are identified. Although the use of RFID tracking has expanded in the USA, it is still not widely adopted. However, In other cases there has been not mix-up of embryos or gametes, but the intentional use of embryos of another couple or gamete donor, without informed consent of parents, both: receptors or donors. Some of these cases are taking a legal and judicial course.
Preimplantation genetic diagnosis or screening
Another concern is that people will screen in or out for particular traits, using preimplantation genetic diagnosis (PGD) or preimplantation genetic screening. For example, a deaf British couple, Tom and Paula Lichy, have petitioned to create a deaf baby using IVF. Some medical ethicists have been very critical of this approach. Jacob M. Appel wrote that "intentionally culling out blind or deaf embryos might prevent considerable future suffering, while a policy that allowed deaf or blind parents to select for such traits intentionally would be far more troublesome."
This concept of decisively altering genes has coined the concept of the Designer Baby. Currently, PGD can alter some physical and health attributes, and projections for the future power of PGD in its ability to create the ideal human has raised many ethical issues. Projections for societal repercussions include changing the realm athletics, creating human weapons, and exchanging autonomy over one’s life course for predesignation. Also, with a limited view of the future, it is difficult to alter a human’s genetic makeup without knowing full repercussions. For example, through gene therapy, a lab was able to make rats lose weight, but the long-term effects of the gene manipulation lead to worry of toxin production and too much weight loss. To prevent some of these issues from arising, scientists work towards stabilising the entire process to make it safer before applying a higher degree of gene modification to the human embryos in IVF.
Autonomy and Tissue Ownership
For those who believe that human life begins at the moment of conception, this belief also suggests that human rights are given at that time. If human rights are given in this embryonic stage, then a surplus of ethical issues arise from manipulating the embryo in the realm of tissue ownership. In the long run, if implanted into a female and born, the embryo becomes an adult and has to now live with the genetic modifications chosen for them through the process of IVF. Unfortunately, in this base, cellular state, consent for gene manipulation is impossible. This leads to decision making by the parents. Rightful parental ownership over the embryo is only in the short-run and means that they control the embryos biological future. Consent over tissue ownership has been an issue for decades and can have legal repercussions. In the case of Henrietta Lacks, researchers lacked patient consent to use her tissues in genetic research, and this led to many legal issues on the family’s right to profit from the use of her cells. Decisiveness over autonomy is necessary in the case of IVF to avoid long run issues and give people their full rights of humanity.
Profit desire of the industry
Many people do not oppose the IVF practice itself (i.e. the creating of a pregnancy through "artificial" ways) but are highly critical of the current state of the present day industry. Such individuals argue that the industry has now become a multibillion-dollar industry, which is widely unregulated and prone to serious abuses in the desire of practitioners to obtain profit. For instance, in 2008, a California physician transferred 12 embryos to a woman who gave birth to octuplets (see Suleman octuplets). This has made international news, and had led to accusations that many doctors are willing to seriously endanger the health and even life of women in order to gain money. Robert Winston, professor of fertility studies at Imperial College London, had called the industry "corrupt" and "greedy" saying that "One of the major problems facing us in healthcare is that IVF has become a massive commercial industry," and that "What has happened, of course, is that money is corrupting this whole technology", and accused authorities of failing to protect couples from exploitation "The regulatory authority has done a consistently bad job. It's not prevented the exploitation of women, it's not put out very good information to couples, it's not limited the number of unscientific treatments people have access to". The IVF industry can thus be seen as an example of what social scientists are describing as an increasing trend towards a market-driven construction of health, medicine and the human body.
As the science progresses, the industry is further driven by money in that researchers and innovators enter into the fight over patents and intellectual property rights. The Copyright Clause in the US Constitution protects innovator’s rights to their respective work in attempts to promote scientific progress. Essentially, this lawful protection gives incentive to the innovators by providing them a temporary monopoly over their respective work. In the IVF industry, already incredibly expensive for patients, patents risk even higher prices for the patients to receive the procedure as they have to also cover the costs of protected works. For example, company 23andMe has patented a process used to calculate probability of gene inheritance. While this innovation could help many, the company retains sole right to administer it and thus does not have economic competition. Lack of economic competition leads to higher prices of products.
The industry has been accused of making unscientific claims, and distorting facts relating to infertility, in particular through widely exaggerated claims about how common infertility is in society, in an attempt to get as many couples as possible and as soon as possible to try treatments (rather than trying to conceive naturally for a longer time). This risks removing infertility from its social context and reducing the experience to a simple biological malfunction, which not only can be treated through bio-medical procedures, but should be treated by them. Indeed, there are serious concerns about the overuse of treatments, for instance Dr Sami David, a fertility specialist and one of the pioneers of the early days of the IVF treatments, has expressed disappointment over the current state of the industry, and said many procedures are unnecessary; he said: "It's being the first choice of treatment rather than the last choice. When it was first opening up in late 1970s, early 80s, it was meant to be the last resort. Now it's a first resort. I think that's an injustice to women. I also think it can harm women in the long run." IVF thus raises ethical issues concerning the abuse of bio-medical facts to ‘sell’ corrective procedures and treatments for conditions that deviate from a constructed ideal of the ‘healthy’ or ‘normal’ body i.e., fertile females and males with reproductive systems capable of co-producing offspring.
Pregnancy past menopause
Although menopause is a natural barrier to further conception, IVF has allowed women to be pregnant in their fifties and sixties. Women whose uteruses have been appropriately prepared receive embryos that originated from an egg of an egg donor. Therefore, although these women do not have a genetic link with the child, they have an emotional link through pregnancy and childbirth. In many cases the genetic father of the child is the woman's partner. Even after menopause the uterus is fully capable of carrying out a pregnancy.
Allowing women to get pregnant past the natural time can factor into issues of overpopulation. Through the PGD, children born through IVF would credibly have higher life expectancy rates due to eliminated diseases. So increasing the amount of women who are able to bear children increases the population growth rate, while PGD in IVF decreases the death rate, resulting in an increasing population.
Same-sex couples, single and unmarried parents
A 2009 statement from the ASRM found no persuasive evidence that children are harmed or disadvantaged solely by being raised by single parents, unmarried parents, or homosexual parents. It did not support restricting access to assisted reproductive technologies on the basis of a prospective parent's marital status or sexual orientation.
Ethical concerns include reproductive rights, the welfare of offspring, nondiscrimination against unmarried individuals, homosexual, and professional autonomy.
A recent controversy in California focused on the question of whether physicians opposed to same-sex relationships should be required to perform IVF for a lesbian couple. Guadalupe T. Benitez, a lesbian medical assistant from San Diego, sued doctors Christine Brody and Douglas Fenton of the North Coast Women's Care Medical Group after Brody told her that she had "religious-based objections to treating her and homosexuals in general to help them conceive children by artificial insemination," and Fenton refused to authorise a refill of her prescription for the fertility drug Clomid on the same grounds. The California Medical Association had initially sided with Brody and Fenton, but the case, North Coast Women's Care Medical Group v. Superior Court, was decided unanimously by the California State Supreme Court in favour of Benitez on 19 August 2008.
Nadya Suleman came to international attention after having twelve embryos implanted, eight of which survived, resulting in eight newborns being added to her existing six-child family. The Medical Board of California sought to have fertility doctor Michael Kamrava, who treated Suleman, stripped of his licence. State officials allege that performing Suleman's procedure is evidence of unreasonable judgment, substandard care, and a lack of concern for the eight children she would conceive and the six she was already struggling to raise. On 1 June 2011 the Medical Board issued a ruling that Kamrava's medical licence be revoked effective 1 July 2011.
Anonymous donors
Some children conceived by IVF using anonymous donors report being troubled over not knowing about their donor parent as well any genetic relatives they may have and their family history.
Alana Stewart, who was conceived using donor sperm, began an online forum for donor children called AnonymousUS in 2010. The forum welcomes the viewpoints of anyone involved in the IVF process. Olivia Pratten, a donor-conceived Canadian, sued the province of British Columbia for access to records on her donor father's identity in 2008. "I’m not a treatment, I’m a person, and those records belong to me,” Pratten said. In May 2012, a court ruled in Pratten's favour, agreeing that the laws at the time discriminated against donor children and making anonymous sperm and egg donation in British Columbia illegal.
In the U.K., Sweden, Norway, Germany, Italy, New Zealand, and some Australian states, donors are not paid and cannot be anonymous.
In 2000, a website called Donor Sibling Registry was created to help biological children with a common donor connect with each other.
In 2012, a documentary called Anonymous Father's Day was released that focuses on donor-conceived children.
Unwanted embryos
During the selection and transfer phases many embryos may be discarded in favour of others. This selection may be based on criteria such as genetic disorders or the sex. One of the earliest cases of special gene selection through IVF was the case of the Collins family in the 1990s, who selected the sex of their child. The ethic issues remain unresolved as no consensus exists in science, religion, and philosophy on when a human embryo should be recognised as a person. For those who believe that this is at the moment of conception, IVF becomes a moral question when multiple eggs are fertilised, begin development, and only a few are chosen for implantation.
If IVF were to involve the fertilisation of only a single egg, or at least only an amount that will be implanted, then this would not be an issue. However, this has the chance of increasing costs dramatically as only a few eggs can be attempted at a time. As a result, the couple must decide what to do with these extra embryos. Depending on their view of the embryo’s humanity or the chance the couple will want to try to have another child, the couple has multiple options for dealing with these extra embryos. Couples can choose to keep them frozen, donate them to other infertile couples, thaw them, or donate them to medical research. Keeping them frozen costs money, donating them does not ensure they will survive, thawing them renders them immediately unviable, and medical research results in their termination. In the realm of medical research, the couple is not necessarily told what the embryos will be used for, and as a result, some can be used in stem cell research, a field perceived to have ethical issues.
Religious response
The Roman Catholic Church opposes all kinds of assisted reproductive technology and artificial contraception, asserting they separate the procreative goal of marital sex from the goal of uniting married couples. The Roman Catholic Church permits the use of a small number of reproductive technologies and contraceptive methods like natural family planning, which involves charting ovulation times. The church allows other forms of reproductive technologies that allow conception to take place from normative sexual intercourse, such as a fertility lubricant. Pope Benedict XVI had publicly re-emphasised the Catholic Church's opposition to in vitro fertilisation, claiming it replaces love between a husband and wife. The Catechism of the Catholic Church claims that Natural law teaches that reproduction has an "inseparable connection" to sexual union of married couples. In addition, the church opposes IVF because it might cause disposal of embryos; in Catholicism, an embryo is viewed as an individual with a soul that must be treated as a person. The Catholic Church maintains that it is not objectively evil to be infertile, and advocates adoption as an option for such couples who still wish to have children.
Hindus welcomed the IVF as gift for those who can't bear child and termed doctors related to IVF doing punya as there are several characters who were claimed to be born without intercourse, mainly Karna and five Pandavas.
Regarding the response to IVF of Islam, the conclusions of Gad El-Hak Ali Gad El-Hak's ART fatwa include that:
Within the Orthodox Jewish community the concept is debated as there is little precedent in traditional Jewish legal textual sources. Regarding laws of sexuality, religious challenges include masturbation (which may be regarded as “seed wasting”), laws related to sexual activity and menstruation (niddah) and the specific laws regarding intercourse. An additional major issue is that of establishing paternity and lineage. For a baby conceived naturally, the father’s identity is determined by a legal presumption (chazakah) of legitimacy: rov bi'ot achar ha'baal - a woman's sexual relations are assumed to be with her husband. Regarding an IVF child, this assumption does not exist and as such Rabbi Eliezer Waldenberg (among others) requires an outside supervisor to positively identify the father. Reform Judaism has generally approved in vitro fertilisation.
Society and culture
Many people of sub-Saharan Africa choose to foster their children to infertile women. IVF enables these infertile women to have their own children, which imposes new ideals to a culture in which fostering children is seen as both natural and culturally important. Many infertile women are able to earn more respect in their society by taking care of the children of other mothers, and this may be lost if they choose to use IVF instead. As IVF is seen as unnatural, it may even hinder their societal position as opposed to making them equal with fertile women. It is also economically advantageous for infertile women to raise foster children as it gives these children greater ability to access resources that are important for their development and also aids the development of their society at large. If IVF becomes more popular without the birth rate decreasing, there could be more large family homes with fewer options to send their newborn children. This could result in an increase of orphaned children and/or a decrease in resources for the children of large families. This would ultimately stifle the children's and the community's growth.
Emotional involvement
Studies have indicated that IVF mothers show greater emotional involvement with their child, and they enjoy motherhood more than mothers by natural conception. Similarly, studies have indicated that IVF fathers express more warmth and emotional involvement than fathers by adoption and natural conception and enjoy fatherhood more. Some IVF parents become overly involved with their children.
Men and IVF
Research has shown that men largely view themselves as ‘passive’ contributors since they have ‘less physical involvement' in IVF treatment. Despite this, many men feel distressed after seeing the toll of hormonal injections and ongoing physical intervention on their partner. Fertility was found to be a significant factor in a man’s perception of his masculinity, driving many to keep the treatment a secret. In cases where the men did share that he and his partner were undergoing IVF, they reported to have been teased, mainly by other men, although some viewed this as an affirmation of support and friendship. For others, this led to feeling socially isolated. In comparison with women, men showed less deterioration in mental health in the years following a failed treatment. However many men did feel guilt, disappointment and inadequacy, stating that they were simply trying to provide an ‘emotional rock’ for their partners.
Availability and utilisation
High costs keep IVF out of reach for many developing countries, but research by the Genk Institute for Fertility Technology, in Belgium, claim to have found a much lower cost methodology (about 90% reduction) with similar efficacy, which may be suitable for some fertility treatment. Moreover, the laws of many countries permit IVF for only single women, lesbian couples, and persons participating in surrogacy arrangements. Using PGD gives members of these select demographic groups disproportionate access to a means of creating a child possessing characteristics that they consider "ideal," raising issues of equal opportunity for both the parents'/parent's and the child's generation. Many fertile couples now demand equal access to embryonic screening so that their child can be just as healthy as one created through IVF. Mass use of PGD, especially as a means of population control or in the presence of legal measures related to population or demographic control, can lead to intentional or unintentional demographic effects such as the skewed live-birth sex ratios seen in communist China following implementation of its one-child policy.
USA
In the USA, overall availability of IVF in 2005 was 2.5 IVF physicians per 100,000 population, and utilisation was 236 IVF cycles per 100,000. Utilisation highly increases with availability and IVF insurance coverage, and to a significant extent also with percentage of single persons and median income. In the USA 126 procedures are performed per million people per year. In the USA an average cycle, from egg retrieval to embryo implantation, costs $12,400, and insurance companies that do cover treatment, even partially, usually cap the number of cycles they pay for.
The cost of IVF rather reflects the costliness of the underlying healthcare system than the regulatory or funding environment, and ranges, on average for a standard IVF cycle and in 2006 United States dollars, between $12,500 in the United States to $4,000 in Japan. In Ireland, IVF costs around €4,000, with fertility drugs, if required, costing up to €3,000. The cost per live birth is highest in the United States ($41,000) and United Kingdom ($40,000) and lowest in Scandinavia and Japan (both around $24,500).
Many fertility clinics in the United States limit the upper age at which women are eligible for IVF to 50 or 55 years. These cut-offs make it difficult for women older than fifty-five to utilise the procedure.
Australia
In Australia, the average age of women undergoing ART treatment is 35.5 years among those using their own eggs (one in four being 40 or older) and 40.5 years among those using donated eggs.
Cameroon
Ernestine Gwet Bell supervised the first Cameroonian child born through IVF in 1998.
Israel
Israel has the highest rate of IVF in the world, with 1657 procedures performed per million people per year. The second highest rate is in Iceland, with 899 procedures per million people per year. Israel provides unlimited free in vitro procedures for its citizens for up to two children per woman under 45 years of age. In other countries the coverage of such procedures is limited if it exists at all. The Israeli Health Ministry says it spends roughly $3450 per procedure.
United Kingdom
Availability of IVF in England is determined by Clinical commissioning groups. The National Institute for Health and Care Excellence (NICE) recommends up to 3 cycles of treatment for women under 40 and one cycle for some women aged between 40 and 42, but financial pressure has eroded compliance with this recommendation. CCGs in Essex, Bedfordshire and Somerset have reduced funding to one cycle, or none, and it is expected that reductions will become more widespread. Funding may be available in “exceptional circumstances” – for example if a male partner has a transmittable infection or one partner is affected by cancer treatment. According to the campaign group Fertility Fairness at the end of 2014 every CCG in England was funding at least one cycle of IVF". Prices paid by the NHS in England varied between under £3,000 to more than £6,000 in 2014/5. In February 2013, the cost of implementing the NICE guidelines for IVF along with other treatments for infertility was projected to be £236,000 per year per 100,000 members of the population.
Legal status
Government agencies in China passed bans on the use of IVF in 2003 by unmarried women or by couples with certain infectious diseases.
Sunni Muslim nations generally allow IVF between married couples when conducted with their own respective sperm and eggs, but not with donor eggs from other couples. But Iran, which is Shi'a Muslim, has a more complex scheme. Iran bans sperm donation but allows donation of both fertilised and unfertilised eggs. Fertilised eggs are donated from married couples to other married couples, while unfertilised eggs are donated in the context of mut'ah or temporary marriage to the father.
By 2012 Costa Rica was the only country in the world with a complete ban on IVF technology, it having been ruled unconstitutional by the nation's Supreme Court because it "violated life." Costa Rica had been the only country in the western hemisphere that forbade IVF. A law project sent reluctantly by the government of President Laura Chinchilla was rejected by parliament. President Chinchilla has not publicly stated her position on the question of IVF. However, given the massive influence of the Catholic Church in her government any change in the status quo seems very unlikely. In spite of Costa Rican government and strong religious opposition, the IVF ban has been struck down by the Inter-American Court of Human Rights in a decision of 20 December 2012. The court said that a long-standing Costa Rican guarantee of protection for every human embryo violated the reproductive freedom of infertile couples because it prohibited them from using IVF, which often involves the disposal of embryos not implanted in a patient’s uterus. On 10 September 2015, President Luis Guillermo Solís signed a decree legalising in-vitro fertilisation. The decree was added to the country's official gazette on 11 September. Opponents of the practice have since filed a lawsuit before the country's Constitutional Court.
All major restrictions on single but infertile women using IVF were lifted in Australia in 2002 after a final appeal to the Australian High Court was rejected on procedural grounds in the Leesa Meldrum case. A Victorian federal court had ruled in 2000 that the existing ban on all single women and lesbians using IVF constituted sex discrimination. Victoria's government announced changes to its IVF law in 2007 eliminating remaining restrictions on fertile single women and lesbians, leaving South Australia as the only state maintaining them.
Federal regulations in the United States include screening requirements and restrictions on donations, but generally do not affect sexually intimate partners. However, doctors may be required to provide treatments due to nondiscrimination laws, as for example in California. The US state of Tennessee proposed a bill in 2009 that would have defined donor IVF as adoption. During the same session another bill proposed barring adoption from any unmarried and cohabitating couple, and activist groups stated that passing the first bill would effectively stop unmarried people from using IVF. Neither of these bills passed.