
 | ||
IUPAC ID (2E,4E,6E,8E)-3,7-dimethyl-9-(2,6,6-trimethylcyclohexen-1-yl)nona-2,4,6,8-tetraen-1-ol | ||
Vitamin A is a group of unsaturated nutritional organic compounds that includes retinol, retinal, retinoic acid, and several provitamin A carotenoids (most notably beta-carotene). Vitamin A has multiple functions: it is important for growth and development, for the maintenance of the immune system and good vision. Vitamin A is needed by the retina of the eye in the form of retinal, which combines with protein opsin to form rhodopsin, the light-absorbing molecule necessary for both low-light (scotopic vision) and color vision. Vitamin A also functions in a very different role as retinoic acid (an irreversibly oxidized form of retinol), which is an important hormone-like growth factor for epithelial and other cells.
Contents
- Deficiency
- Vitamin A supplementation
- Side effects
- History
- Equivalencies of retinoids and carotenoids IU
- Recommended dietary allowance
- Metabolic functions
- Vision
- Gene transcription
- Dermatology
- Retinalretinol versus retinoic acid
- Vitamin A and derivatives in medical use
- References
In foods of animal origin, the major form of vitamin A is an ester, primarily retinyl palmitate, which is converted to retinol (chemically an alcohol) in the small intestine. The retinol form functions as a storage form of the vitamin, and can be converted to and from its visually active aldehyde form, retinal.
All forms of vitamin A have a beta-ionone ring to which an isoprenoid chain is attached, called a retinyl group. Both structural features are essential for vitamin activity. The orange pigment of carrots (beta-carotene) can be represented as two connected retinyl groups, which are used in the body to contribute to vitamin A levels. Alpha-carotene and gamma-carotene also have a single retinyl group, which give them some vitamin activity. None of the other carotenes have vitamin activity. The carotenoid beta-cryptoxanthin possesses an ionone group and has vitamin activity in humans.
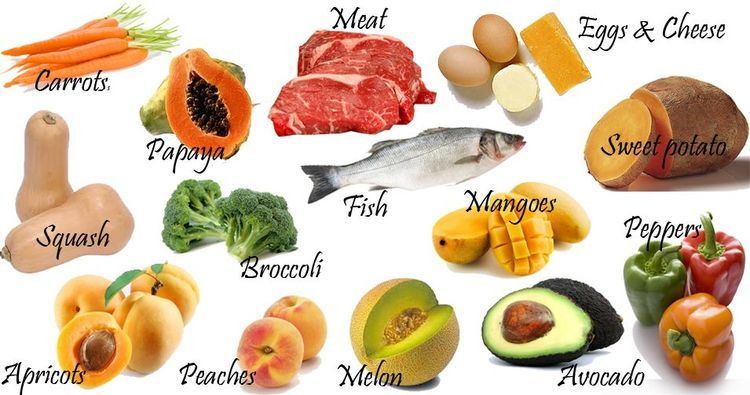
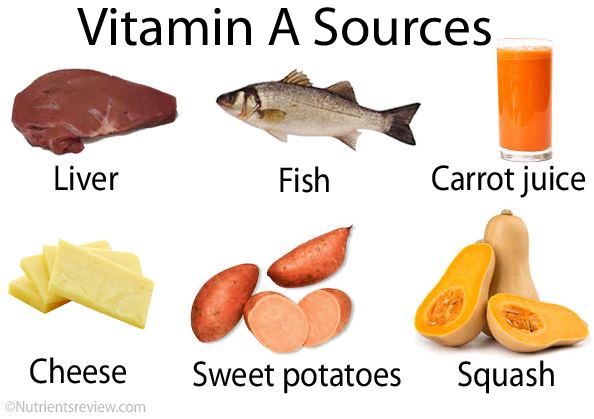
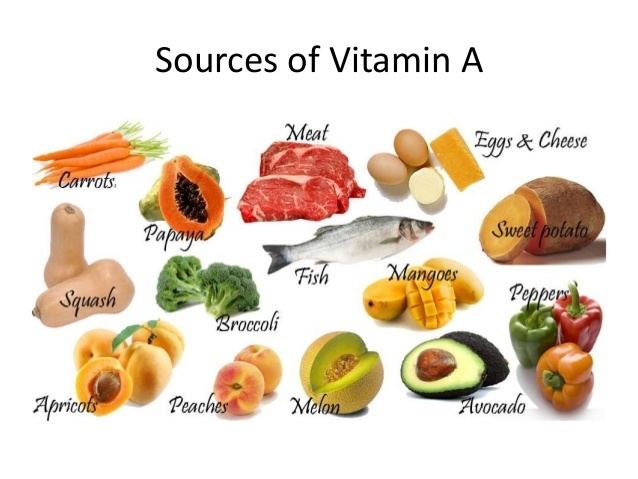
Vitamin A can be found in two principal forms in foods:
Deficiency
Vitamin A deficiency is estimated to affect approximately one third of children under the age of five around the world. It is estimated to claim the lives of 670,000 children under five annually. Approximately 250,000–500,000 children in developing countries become blind each year owing to vitamin A deficiency, with the highest prevalence in Southeast Asia and Africa. Vitamin A deficiency is "the leading cause of preventable childhood blindness," according to UNICEF. It also increases the risk of death from common childhood conditions such as diarrhea. UNICEF regards addressing vitamin A deficiency as critical to reducing child mortality, the fourth of the United Nations' Millennium Development Goals.
Vitamin A deficiency can occur as either a primary or a secondary deficiency. A primary vitamin A deficiency occurs among children and adults who do not consume an adequate intake of provitamin A carotenoids from fruits and vegetables or preformed vitamin A from animal and dairy products. Early weaning from breastmilk can also increase the risk of vitamin A deficiency.
Secondary vitamin A deficiency is associated with chronic malabsorption of lipids, impaired bile production and release, and chronic exposure to oxidants, such as cigarette smoke, and chronic alcoholism. Vitamin A is a fat-soluble vitamin and depends on micellar solubilization for dispersion into the small intestine, which results in poor use of vitamin A from low-fat diets. Zinc deficiency can also impair absorption, transport, and metabolism of vitamin A because it is essential for the synthesis of the vitamin A transport proteins and as the cofactor in conversion of retinol to retinal. In malnourished populations, common low intakes of vitamin A and zinc increase the severity of vitamin A deficiency and lead physiological signs and symptoms of deficiency. A study in Burkina Faso showed major reduction of malaria morbidity with combined vitamin A and zinc supplementation in young children.

Due to the unique function of retinal as a visual chromophore, one of the earliest and specific manifestations of vitamin A deficiency is impaired vision, particularly in reduced light – night blindness. Persistent deficiency gives rise to a series of changes, the most devastating of which occur in the eyes. Some other ocular changes are referred to as xerophthalmia. First there is dryness of the conjunctiva (xerosis) as the normal lacrimal and mucus-secreting epithelium is replaced by a keratinized epithelium. This is followed by the build-up of keratin debris in small opaque plaques (Bitot's spots) and, eventually, erosion of the roughened corneal surface with softening and destruction of the cornea (keratomalacia) and leading to total blindness. Other changes include impaired immunity (increased risk of ear infections, urinary tract infections, Meningococcal disease), hyperkeratosis (white lumps at hair follicles), keratosis pilaris and squamous metaplasia of the epithelium lining the upper respiratory passages and urinary bladder to a keratinized epithelium. With relations to dentistry, a deficiency in Vitamin A leads to enamel hypoplasia.
Adequate supply, but not excess vitamin A, is especially important for pregnant and breastfeeding women for normal fetal development and in breastmilk. Deficiencies cannot be compensated by postnatal supplementation. Excess vitamin A, which is most common with high dose vitamin supplements, can cause birth defects and therefore should not exceed recommended daily values.

Vitamin A metabolic inhibition as a result of alcohol consumption during pregnancy is the elucidated mechanism for fetal alcohol syndrome and is characterized by teratogenicity closely matching maternal vitamin A deficiency.
Vitamin A supplementation
Global efforts to support national governments in addressing vitamin A deficiency are led by the Global Alliance for Vitamin A (GAVA), which is an informal partnership between A2Z, the Canadian International Development Agency, Helen Keller International, the Micronutrient Initiative, UNICEF, USAID, and the World Bank. Joint GAVA activity is coordinated by the Micronutrient Initiative.
While strategies include intake of vitamin A through a combination of breast feeding and dietary intake, delivery of oral high-dose supplements remain the principal strategy for minimizing deficiency. A meta-analysis of 43 studies showed that vitamin A supplementation of children under five who are at risk of deficiency reduces mortality by up to 24%. About 75% of the vitamin A required for supplementation activity by developing countries is supplied by the Micronutrient Initiative with support from the Canadian International Development Agency. Food fortification approaches are becoming increasingly feasible but cannot yet ensure coverage levels.
The World Health Organization estimates that Vitamin A supplementation has averted 1.25 million deaths due to vitamin A deficiency in 40 countries since 1998. In 2008 it was estimated that an annual investment of US$60 million in vitamin A and zinc supplementation combined would yield benefits of more than US$1 billion per year, with every dollar spent generating benefits of more than US$17. These combined interventions were ranked by the Copenhagen Consensus 2008 as the world’s best development investment.
Observational studies of pregnant women in sub-Saharan Africa have shown that low serum vitamin A levels are associated with an increased risk of mother-to-child transmission (MTCT) of HIV. Vitamin A is cheap and easily provided through existing health services in low-income settings. It is thus important to determine the effect of routine supplementation of H levels, and because low blood vitamin A levels have been associated with rapid HIV infection and deaths, To identify randomised controlled trials comparing vitamin A supplementation with placebo in known HIV-infected pregnant women, authors searched the Cochrane Library, PubMed, EMBASE, AIDSearch and GATEWAY; checked reference lis,. Authoritative reviews of more recent and better-designed studies have found no relationship between the level of serum maternal and/or infant vitamin A and the likelihood of vertical (MTCT) HIV transmission. of HIV, our trials which enrolled 3033 HIV-infected pregnant women met inclusion criteria. Authors found significant statistical heterogeneity between the three trials with information on MTCT of HIV. Overall, there was no evidence of an effect of antenatal vitamin A supplementation on the risk of MTCT of HIV. However, antenatal vitamin A supplementation significantly improved birth weight, but there was no evidence of an effect on preterm births, stillbirths, deaths by 24 months. Evidence is also lacking on whether vitamin A supplementation for infants up to six months of age reduces infant mortality or morbidity in low- and middle-income countries.
Side effects
Since vitamin A is fat-soluble, disposing of any excesses taken in through diet takes much longer than with water-soluble B vitamins and vitamin C. This allows for toxic levels of vitamin A to accumulate. These toxicities only occur with preformed (retinoid) vitamin A (such as from liver). The carotenoid forms (such as beta-carotene as found in carrots), give no such symptoms, except with supplements and chronic alcoholism, but excessive dietary intake of beta-carotene can lead to carotenodermia, a harmless but cosmetically displeasing orange-yellow discoloration of the skin.
In general, acute toxicity occurs at doses of 25,000 IU/kg of body weight, with chronic toxicity occurring at 4,000 IU/kg of body weight daily for 6–15 months. However, liver toxicities can occur at levels as low as 15,000 IU (4500 micrograms) per day to 1.4 million IU per day, with an average daily toxic dose of 120,000 IU, particularly with excessive consumption of alcohol. In people with renal failure, 4000 IU can cause substantial damage. Children can reach toxic levels at 1,500 IU/kg of body weight.
Excessive vitamin A consumption can lead to nausea, irritability, anorexia (reduced appetite), vomiting, blurry vision, headaches, hair loss, muscle and abdominal pain and weakness, drowsiness, and altered mental status. In chronic cases, hair loss, dry skin, drying of the mucous membranes, fever, insomnia, fatigue, weight loss, bone fractures, anemia, and diarrhea can all be evident on top of the symptoms associated with less serious toxicity. Some of these symptoms are also common to acne treatment with Isotretinoin. Chronically high doses of vitamin A, and also pharmaceutical retinoids such as 13-cis retinoic acid, can produce the syndrome of pseudotumor cerebri. This syndrome includes headache, blurring of vision and confusion, associated with increased intracerebral pressure. Symptoms begin to resolve when intake of the offending substance is stopped.
Chronic intake of 1500 RAE of preformed vitamin A may be associated with osteoporosis and hip fractures because it suppresses bone building while simultaneously stimulating bone breakdown.
High vitamin A intake has been associated with spontaneous bone fractures in animals. Cell culture studies have linked increased bone resorption and decreased bone formation with high intakes. This interaction may occur because vitamins A and D may compete for the same receptor and then interact with parathyroid hormone, which regulates calcium. Indeed, a study by Forsmo et al. shows a correlation between low bone mineral density and too high intake of vitamin A. Sufficiently high levels of vitamin D may be protective against the bone density lowering effects of high vitamin A, while inadequate levels of vitamin D may exacerbate those effects.
Toxic effects of vitamin A have been shown to significantly affect developing fetuses. Therapeutic doses used for acne treatment have been shown to disrupt cephalic neural cell activity. The fetus is particularly sensitive to vitamin A toxicity during the period of organogenesis.
Hepatic (liver) injury has been found in human and animal studies where consumption of alcohol is paired with high dose vitamin A and beta-carotene supplementation.
Researchers have succeeded in creating water-miscible vitamin A, but one human trial reported water-miscible vitamin A was approximately 10 times as toxic as fat-soluble vitamin. A 2006 study found children given water-miscible vitamin A and D, which are typically fat-soluble, suffer from asthma twice as much as a control group supplemented with the fat-soluble vitamins.
In some studies, the use of Vitamin A supplements has been linked to an increased rate of mortality.
History
The discovery of vitamin A may have stemmed from research dating back to 1816, when physiologist François Magendie observed that dogs deprived of nutrition developed corneal ulcers and had a high mortality rate. In 1912, Frederick Gowland Hopkins demonstrated that unknown accessory factors found in milk, other than carbohydrates, proteins, and fats were necessary for growth in rats. Hopkins received a Nobel Prize for this discovery in 1929. By 1913, one of these substances was independently discovered by Elmer McCollum and Marguerite Davis at the University of Wisconsin–Madison, and Lafayette Mendel and Thomas Burr Osborne at Yale University who studied the role of fats in the diet. McCollum and Davis ultimately received credit because they submitted their paper three weeks before Mendel and Osborne. Both papers appeared in the same issue of the Journal of Biological Chemistry in 1913. The "accessory factors" were termed "fat soluble" in 1918 and later "vitamin A" in 1920. In 1919, Harry Steenbock (University of Wisconsin–Madison) proposed a relationship between yellow plant pigments (beta-carotene) and vitamin A. In 1931, Swiss chemist Paul Karrer described the chemical structure of vitamin A. Vitamin A was first synthesized in 1947 by two Dutch chemists, David Adriaan van Dorp and Jozef Ferdinand Arens.
Equivalencies of retinoids and carotenoids (IU)
As some carotenoids can be converted into vitamin A, attempts have been made to determine how much of them in the diet is equivalent to a particular amount of retinol, so that comparisons can be made of the benefit of different foods. The situation can be confusing because the accepted equivalences have changed. For many years, a system of equivalencies in which an international unit (IU) was equal to 0.3 μg of retinol, 0.6 μg of β-carotene, or 1.2 μg of other provitamin-A carotenoids was used. Later, a unit called retinol equivalent (RE) was introduced. Prior to 2001, one RE corresponded to 1 μg retinol, 2 μg β-carotene dissolved in oil (it is only partly dissolved in most supplement pills, due to very poor solubility in any medium), 6 μg β-carotene in normal food (because it is not absorbed as well as when in oils), and 12 μg of either α-carotene, γ-carotene, or β-cryptoxanthin in food.
Newer research has shown that the absorption of provitamin-A carotenoids is only half as much as previously thought. As a result, in 2001 the US Institute of Medicine recommended a new unit, the retinol activity equivalent (RAE). Each μg RAE corresponds to 1 μg retinol, 2 μg of β-carotene in oil, 12 μg of "dietary" beta-carotene, or 24 μg of the three other dietary provitamin-A carotenoids.
Because the conversion of retinol from provitamin carotenoids by the human body is actively regulated by the amount of retinol available to the body, the conversions apply strictly only for vitamin A-deficient humans. The absorption of provitamins depends greatly on the amount of lipids ingested with the provitamin; lipids increase the uptake of the provitamin.
The conclusion that can be drawn from the newer research is that fruits and vegetables are not as useful for obtaining vitamin A as was thought; in other words, the IUs that these foods were reported to contain were worth much less than the same number of IUs of fat-dissolved oils and (to some extent) supplements. This is important for vegetarians, as night blindness is prevalent in countries where little meat or vitamin A-fortified foods are available.
A sample vegan diet for one day that provides sufficient vitamin A has been published by the Food and Nutrition Board (page 120). On the other hand, reference values for retinol or its equivalents, provided by the National Academy of Sciences, have decreased. The RDA (for men) of 1968 was 5000 IU (1500 μg retinol). In 1974, the RDA was set to 1000 RE (1000 μg retinol), whereas now the Dietary Reference Intake is 900 RAE (900 μg or 3000 IU retinol). This is equivalent to 1800 μg of β-carotene supplement (3000 IU) or 10800 μg of β-carotene in food (18000 IU).
Recommended dietary allowance
Vitamin A
Dietary Reference Intakes:
Metabolic functions
Vitamin A plays a role in a variety of functions throughout the body, such as:
Vision
The role of vitamin A in the visual cycle is specifically related to the retinal form. Within the eye, 11-cis-retinal is bound to the protein "opsin" to form rhodopsin in rods and iodopsin (cones) at conserved lysine residues. As light enters the eye, the 11-cis-retinal is isomerized to the all-"trans" form. The all-"trans" retinal dissociates from the opsin in a series of steps called photo-bleaching. This isomerization induces a nervous signal along the optic nerve to the visual center of the brain. After separating from opsin, the all-"trans"-retinal is recycled and converted back to the 11-"cis"-retinal form by a series of enzymatic reactions. In addition, some of the all-"trans" retinal may be converted to all-"trans" retinol form and then transported with an interphotoreceptor retinol-binding protein (IRBP) to the pigment epithelial cells. Further esterification into all-"trans" retinyl esters allow for storage of all-trans-retinol within the pigment epithelial cells to be reused when needed. The final stage is conversion of 11-cis-retinal will rebind to opsin to reform rhodopsin (visual purple) in the retina. Rhodopsin is needed to see in low light (contrast) as well as for night vision. Kühne showed that rhodopsin in the retina is only regenerated when the retina is attached to retinal pigmented epithelium, which provides retinal. It is for this reason that a deficiency in vitamin A will inhibit the reformation of rhodopsin and lead to one of the first symptoms, night blindness.
Gene transcription
Vitamin A, in the retinoic acid form, plays an important role in gene transcription. Once retinol has been taken up by a cell, it can be oxidized to retinal (retinaldehyde) by retinol dehydrogenases and then retinaldehyde can be oxidized to retinoic acid by retinaldehyde dehydrogenases. The conversion of retinaldehyde to retinoic acid is an irreversible step, meaning that the production of retinoic acid is tightly regulated, due to its activity as a ligand for nuclear receptors. The physiological form of retinoic acid (all-trans-retinoic acid) regulates gene transcription by binding to nuclear receptors known as retinoic acid receptors (RARs) which are bound to DNA as heterodimers with retinoid "X" receptors (RXRs). RAR and RXR must dimerize before they can bind to the DNA. RAR will form a heterodimer with RXR (RAR-RXR), but it does not readily form a homodimer (RAR-RAR). RXR, on the other hand, may form a homodimer (RXR-RXR) and will form heterodimers with many other nuclear receptors as well, including the thyroid hormone receptor (RXR-TR), the Vitamin D3 receptor (RXR-VDR), the peroxisome proliferator-activated receptor (RXR-PPAR) and the liver "X" receptor (RXR-LXR). The RAR-RXR heterodimer recognizes retinoic acid response elements (RAREs) on the DNA whereas the RXR-RXR homodimer recognizes retinoid "X" response elements (RXREs) on the DNA; although several RAREs near target genes have been shown to control physiological processes, this has not been demonstrated for RXREs. The heterodimers of RXR with nuclear receptors other than RAR (i.e. TR, VDR, PPAR, LXR) bind to various distinct response elements on the DNA to control processes not regulated by vitamin A. Upon binding of retinoic acid to the RAR component of the RAR-RXR heterodimer, the receptors undergo a conformational change that causes co-repressors to dissociate from the receptors. Coactivators can then bind to the receptor complex, which may help to loosen the chromatin structure from the histones or may interact with the transcriptional machinery. This response can upregulate (or downregulate) the expression of target genes, including Hox genes as well as the genes that encode for the receptors themselves (i.e. RAR-beta in mammals).
Dermatology
Vitamin A, and more specifically, retinoic acid, appears to maintain normal skin health by switching on genes and differentiating keratinocytes (immature skin cells) into mature epidermal cells. Exact mechanisms behind pharmacological retinoid therapy agents in the treatment of dermatological diseases are being researched. For the treatment of acne, the most prescribed retinoid drug is 13-cis retinoic acid (isotretinoin). It reduces the size and secretion of the sebaceous glands. Although it is known that 40 mg of isotretinoin will break down to an equivalent of 10 mg of ATRA — the mechanism of action of the drug (original brand name Accutane) remains unknown and is a matter of some controversy. Isotretinoin reduces bacterial numbers in both the ducts and skin surface. This is thought to be a result of the reduction in sebum, a nutrient source for the bacteria. Isotretinoin reduces inflammation via inhibition of chemotactic responses of monocytes and neutrophils. Isotretinoin also has been shown to initiate remodeling of the sebaceous glands; triggering changes in gene expression that selectively induce apoptosis. Isotretinoin is a teratogen with a number of potential side-effects. Consequently, its use requires medical supervision.
Retinal/retinol versus retinoic acid
Vitamin A deprived rats can be kept in good general health with supplementation of retinoic acid. This reverses the growth-stunting effects of vitamin A deficiency, as well as early stages of xerophthalmia. However, such rats show infertility (in both male and females) and continued degeneration of the retina, showing that these functions require retinal or retinol, which are interconvertible but which cannot be recovered from the oxidized retinoic acid. The requirement of retinol to rescue reproduction in vitamin A deficient rats is now known to be due to a requirement for local synthesis of retinoic acid from retinol in testis and embryos.
Vitamin A and derivatives in medical use
Retinyl palmitate has been used in skin creams, where it is broken down to retinol and ostensibly metabolised to retinoic acid, which has potent biological activity, as described above.
The retinoids (for example, 13-cis-retinoic acid) constitute a class of chemical compounds chemically related to retinoic acid, and are used in medicine to modulate gene functions in place of this compound. Like retinoic acid, the related compounds do not have full vitamin A activity, but do have powerful effects on gene expression and epithelial cell differentiation.
Pharmaceutics utilizing mega doses of naturally occurring retinoic acid derivatives are currently in use for cancer, HIV, and dermatological purposes. At high doses, side-effects are similar to vitamin A toxicity.