
ICD-9-CM 155.1, 156.1 OMIM 615619 | ICD-10 C22.1 ICD-O M8160/3 DiseasesDB 2505 | |
 | ||
Cholangiocarcinoma or bile duct cancer is a form of cancer that is composed of mutated epithelial cells (or cells showing characteristics of epithelial differentiation) that originate in the bile ducts which drain bile from the liver into the small intestine. Other biliary tract cancers include gallbladder cancer and cancer of the ampulla of Vater.
Contents
- Signs and symptoms
- Risk factors
- Pathophysiology
- Diagnosis
- Blood tests
- Abdominal imaging
- Imaging of the biliary tree
- Surgery
- Pathology
- Staging
- Treatment
- Adjuvant chemotherapy and radiation therapy
- Treatment of advanced disease
- Prognosis
- Epidemiology
- Research
- References
Cholangiocarcinoma is a relatively rare neoplasm that is classified as an adenocarcinoma (a cancer that forms glands or secretes significant amounts of mucins). It has an annual incidence rate of 1–2 cases per 100,000 in the Western world, but rates of cholangiocarcinoma have been rising worldwide over the past few decades.
Prominent signs and symptoms of cholangiocarcinoma include abnormal liver function tests, abdominal pain, jaundice, and weight loss. Other symptoms such as generalized itching, fever, and changes in color of stool or urine may also occur. The disease is diagnosed through a combination of blood tests, imaging, endoscopy, and sometimes surgical exploration, with confirmation obtained after a pathologist examines cells from the tumor under a microscope. Known risk factors for cholangiocarcinoma include primary sclerosing cholangitis (an inflammatory disease of the bile ducts), infection with the parasitic liver flukes Opisthorchis viverrini or Clonorchis sinensis, some congenital liver malformations, and exposure to Thorotrast (thorium dioxide), a chemical formerly used in medical imaging. However, most people with cholangiocarcinoma have no identifiable risk factors.
Cholangiocarcinoma is considered to be an incurable and rapidly lethal cancer unless both the primary tumor and any metastases can be fully removed by surgery. No potentially curative treatment exists except surgery, but most people have advanced stage disease at presentation and are inoperable at the time of diagnosis. People with cholangiocarcinoma are generally managed - though not cured - with chemotherapy, radiation therapy, and other palliative care measures. These are also used as additional therapies after surgery in cases where resection has apparently been successful (or nearly so).
Signs and symptoms
The most common physical indications of cholangiocarcinoma are abnormal liver function tests, jaundice (yellowing of the eyes and skin occurring when bile ducts are blocked by tumor), abdominal pain (30%–50%), generalized itching (66%), weight loss (30%–50%), fever (up to 20%), and changes in the color of stool or urine. To some extent, the symptoms depend upon the location of the tumor: patients with cholangiocarcinoma in the extrahepatic bile ducts (outside the liver) are more likely to have jaundice, while those with tumors of the bile ducts within the liver more often have pain without jaundice.
Blood tests of liver function in patients with cholangiocarcinoma often reveal a so-called "obstructive picture," with elevated bilirubin, alkaline phosphatase, and gamma glutamyl transferase levels, and relatively normal transaminase levels. Such laboratory findings suggest obstruction of the bile ducts, rather than inflammation or infection of the liver parenchyma, as the primary cause of the jaundice. CA19-9 is elevated in most cases of cholangiocarcinoma.
Risk factors
Although most patients present without any known risk factors evident, a number of risk factors for the development of cholangiocarcinoma have been described. In the Western world, the most common of these is primary sclerosing cholangitis (PSC), an inflammatory disease of the bile ducts which is closely associated with ulcerative colitis (UC). Epidemiologic studies have suggested that the lifetime risk of developing cholangiocarcinoma for a person with PSC is on the order of 10%–15%, although autopsy series have found rates as high as 30% in this population. The mechanism by which PSC increases the risk of cholangiocarcinoma is not well understood.
Certain parasitic liver diseases may be risk factors as well. Colonization with the liver flukes Opisthorchis viverrini (found in Thailand, Laos PDR, and Vietnam) or Clonorchis sinensis (found in China, Taiwan, eastern Russia, Korea, and Vietnam) has been associated with the development of cholangiocarcinoma. Patients with chronic liver disease, whether in the form of viral hepatitis (e.g. hepatitis B or hepatitis C), alcoholic liver disease, or cirrhosis of the liver due to other causes, are at significantly increased risk of cholangiocarcinoma. HIV infection was also identified in one study as a potential risk factor for cholangiocarcinoma, although it was unclear whether HIV itself or other correlated and confounding factors (e.g. hepatitis C infection) were responsible for the association.
Infection with the bacteria Helicobacter bilis and Helicobacter hepaticus species can cause biliary cancer.
Congenital liver abnormalities, such as Caroli's syndrome (a specific type of five recognized choledochal cysts), have been associated with an approximately 15% lifetime risk of developing cholangiocarcinoma. The rare inherited disorders Lynch syndrome II and biliary papillomatosis have also been found to be associated with cholangiocarcinoma. The presence of gallstones (cholelithiasis) is not clearly associated with cholangiocarcinoma. However, intrahepatic stones (called hepatolithiasis), which are rare in the West but common in parts of Asia, have been strongly associated with cholangiocarcinoma. Exposure to Thorotrast, a form of thorium dioxide which was used as a radiologic contrast medium, has been linked to the development of cholangiocarcinoma as late as 30–40 years after exposure; Thorotrast was banned in the United States in the 1950s due to its carcinogenicity.
Pathophysiology
Cholangiocarcinoma can affect any area of the bile ducts, either within or outside the liver. Tumors occurring in the bile ducts within the liver are referred to as intrahepatic, those occurring in the ducts outside the liver are extrahepatic, and tumors occurring at the site where the bile ducts exit the liver may be referred to as perihilar. A cholangiocarcinoma occurring at the junction where the left and right hepatic ducts meet to form the common hepatic duct may be referred to eponymously as a Klatskin tumor.
Although cholangiocarcinoma is known to have the histological and molecular features of an adenocarcinoma of epithelial cells lining the biliary tract, the actual cell of origin is unknown. Recent evidence has suggested that the initial transformed cell that generates the primary tumor may arise from a pluripotent hepatic stem cell. Cholangiocarcinoma is thought to develop through a series of stages - from early hyperplasia and metaplasia, through dysplasia, to the development of frank carcinoma - in a process similar to that seen in the development of colon cancer. Chronic inflammation and obstruction of the bile ducts, and the resulting impaired bile flow, are thought to play a role in this progression.
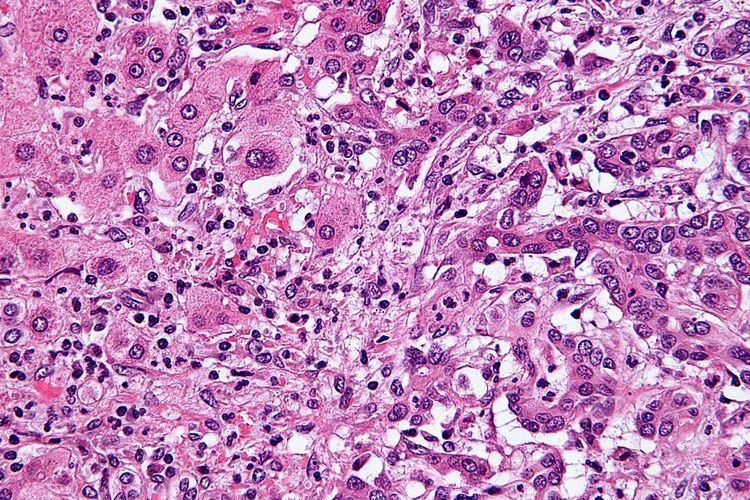
Histologically, cholangiocarcinomas may vary from undifferentiated to well-differentiated. They are often surrounded by a brisk fibrotic or desmoplastic tissue response; in the presence of extensive fibrosis, it can be difficult to distinguish well-differentiated cholangiocarcinoma from normal reactive epithelium. There is no entirely specific immunohistochemical stain that can distinguish malignant from benign biliary ductal tissue, although staining for cytokeratins, carcinoembryonic antigen, and mucins may aid in diagnosis. Most tumors (>90%) are adenocarcinomas.
Diagnosis
Cholangiocarcinoma is definitively diagnosed from tissue, i.e. it is proven by biopsy or examination of the tissue excised at surgery. It may be suspected in a patient with obstructive jaundice. Considering it as the working diagnosis may be challenging in patients with primary sclerosing cholangitis (PSC); such patients are at high risk of developing cholangiocarcinoma, but the symptoms may be difficult to distinguish from those of PSC. Furthermore, in patients with PSC, such diagnostic clues as a visible mass on imaging or biliary ductal dilatation may not be evident.
Blood tests
There are no specific blood tests that can diagnose cholangiocarcinoma by themselves. Serum levels of carcinoembryonic antigen (CEA) and CA19-9 are often elevated, but are not sensitive or specific enough to be used as a general screening tool. However, they may be useful in conjunction with imaging methods in supporting a suspected diagnosis of cholangiocarcinoma.
Abdominal imaging
Ultrasound of the liver and biliary tree is often used as the initial imaging modality in patients with suspected obstructive jaundice. Ultrasound can identify obstruction and ductal dilatation and, in some cases, may be sufficient to diagnose cholangiocarcinoma. Computed tomography (CT) scanning may also play an important role in the diagnosis of cholangiocarcinoma.
Imaging of the biliary tree
While abdominal imaging can be useful in the diagnosis of cholangiocarcinoma, direct imaging of the bile ducts is often necessary. Endoscopic retrograde cholangiopancreatography (ERCP), an endoscopic procedure performed by a gastroenterologist or specially trained surgeon, has been widely used for this purpose. Although ERCP is an invasive procedure with attendant risks, its advantages include the ability to obtain biopsies and to place stents or perform other interventions to relieve biliary obstruction. Endoscopic ultrasound can also be performed at the time of ERCP and may increase the accuracy of the biopsy and yield information on lymph node invasion and operability. As an alternative to ERCP, percutaneous transhepatic cholangiography (PTC) may be utilized. Magnetic resonance cholangiopancreatography (MRCP) is a non-invasive alternative to ERCP. Some authors have suggested that MRCP should supplant ERCP in the diagnosis of biliary cancers, as it may more accurately define the tumor and avoids the risks of ERCP.
Surgery
Surgical exploration may be necessary to obtain a suitable biopsy and to accurately stage a patient with cholangiocarcinoma. Laparoscopy can be used for staging purposes and may avoid the need for a more invasive surgical procedure, such as laparotomy, in some patients. Surgery is also the only curative option for cholangiocarcinoma, although it is limited to patients with early-stage disease.
Pathology
Histologically, cholangiocarcinomas are classically well to moderately differentiated adenocarcinomas. Immunohistochemistry is useful in the diagnosis and may be used to help differentiate a cholangiocarcinoma from hepatocellular carcinoma and metastasis of other gastrointestinal tumors. Cytological scrapings are often nondiagnostic, as these tumors typically have a desmoplastic stroma and, therefore, do not release diagnostic tumor cells with scrapings.
Staging
Although there are at least three staging systems for cholangiocarcinoma (e.g. those of Bismuth, Blumgart, and the American Joint Committee on Cancer), none have been shown to be useful in predicting survival. The most important staging issue is whether the tumor can be surgically removed, or whether it is too advanced for surgical treatment to be successful. Often, this determination can only be made at the time of surgery.
General guidelines for operability include:
Treatment
Cholangiocarcinoma is considered to be an incurable and rapidly lethal disease unless all the tumors can be fully resected (that is, cut out surgically). Since the operability of the tumor can only be assessed during surgery in most cases, a majority of patients undergo exploratory surgery unless there is already a clear indication that the tumor is inoperable. However, the Mayo Clinic has reported significant success treating early bile duct cancer with liver transplantation using a protocolized approach and strict selection criteria.
Adjuvant therapy followed by liver transplantation may have a role in treatment of certain unresectable cases.
Adjuvant chemotherapy and radiation therapy
If the tumor can be removed surgically, patients may receive adjuvant chemotherapy or radiation therapy after the operation to improve the chances of cure. If the tissue margins are negative (i.e. the tumor has been totally excised), adjuvant therapy is of uncertain benefit. Both positive and negative results have been reported with adjuvant radiation therapy in this setting, and no prospective randomized controlled trials have been conducted as of March 2007. Adjuvant chemotherapy appears to be ineffective in patients with completely resected tumors. The role of combined chemoradiotherapy in this setting is unclear. However, if the tumor tissue margins are positive, indicating that the tumor was not completely removed via surgery, then adjuvant therapy with radiation and possibly chemotherapy is generally recommended based on the available data.
Treatment of advanced disease
The majority of cases of cholangiocarcinoma present as inoperable (unresectable) disease in which case patients are generally treated with palliative chemotherapy, with or without radiotherapy. Chemotherapy has been shown in a randomized controlled trial to improve quality of life and extend survival in patients with inoperable cholangiocarcinoma. There is no single chemotherapy regimen which is universally used, and enrollment in clinical trials is often recommended when possible. Chemotherapy agents used to treat cholangiocarcinoma include 5-fluorouracil with leucovorin, gemcitabine as a single agent, or gemcitabine plus cisplatin, irinotecan, or capecitabine. A small pilot study suggested possible benefit from the tyrosine kinase inhibitor erlotinib in patients with advanced cholangiocarcinoma.
Prognosis
Surgical resection offers the only potential chance of cure in cholangiocarcinoma. For non-resectable cases, the 5-year survival rate is 0% where the disease is inoperable because distal lymph nodes show metastases, and less than 5% in general. Overall median duration of survival is less than 6 months in inoperable, untreated, otherwise healthy patients with tumors involving the liver by way of the intrahepatic bile ducts and hepatic portal vein.
For surgical cases, the odds of cure vary depending on the tumor location and whether the tumor can be completely, or only partially, removed. Distal cholangiocarcinomas (those arising from the common bile duct) are generally treated surgically with a Whipple procedure; long-term survival rates range from 15%–25%, although one series reported a five-year survival of 54% for patients with no involvement of the lymph nodes. Intrahepatic cholangiocarcinomas (those arising from the bile ducts within the liver) are usually treated with partial hepatectomy. Various series have reported survival estimates after surgery ranging from 22%–66%; the outcome may depend on involvement of lymph nodes and completeness of the surgery. Perihilar cholangiocarcinomas (those occurring near where the bile ducts exit the liver) are least likely to be operable. When surgery is possible, they are generally treated with an aggressive approach often including removal of the gallbladder and potentially part of the liver. In patients with operable perihilar tumors, reported 5-year survival rates range from 20%–50%.
The prognosis may be worse for patients with primary sclerosing cholangitis who develop cholangiocarcinoma, likely because the cancer is not detected until it is advanced. Some evidence suggests that outcomes may be improving with more aggressive surgical approaches and adjuvant therapy.
Epidemiology
Cholangiocarcinoma is a relatively rare form of cancer; each year, approximately 2,000 to 3,000 new cases are diagnosed in the United States, translating into an annual incidence of 1–2 cases per 100,000 people. Autopsy series have reported a prevalence of 0.01% to 0.46%. There is a higher prevalence of cholangiocarcinoma in Asia, which has been attributed to endemic chronic parasitic infestation. The incidence of cholangiocarcinoma increases with age, and the disease is slightly more common in men than in women (possibly due to the higher rate of primary sclerosing cholangitis, a major risk factor, in men). The prevalence of cholangiocarcinoma in patients with primary sclerosing cholangitis may be as high as 30%, based on autopsy studies.
Multiple studies have documented a steady increase in the incidence of intrahepatic cholangiocarcinoma over the past several decades; increases have been seen in North America, Europe, Asia, and Australia. The reasons for the increasing occurrence of cholangiocarcinoma are unclear; improved diagnostic methods may be partially responsible, but the prevalence of potential risk factors for cholangiocarcinoma, such as HIV infection, has also been increasing during this time frame.
Research
Some areas of ongoing medical research in cholangiocarcinoma include the use of newer targeted therapies, (such as erlotinib) or photodynamic therapy for treatment, and the techniques to measure the concentration of byproducts of cancer stromal cell formation in the blood for diagnostic purposes.