
Specialty medical genetics ICD-9-CM 751.69 MeSH D015529 | ICD-10 Q44.4 DiseasesDB 2527 | |
 | ||
eMedicine article/172099 article/366004 article/934267 | ||
Choledochal cysts (a.k.a. bile duct cyst) are congenital conditions involving cystic dilatation of bile ducts. They are uncommon in western countries but not as rare in East Asian nations like Japan and China.
Contents
Signs and symptoms
Most patients have symptoms in the first year of life. It is rare for symptoms to be undetected until adulthood, and usually adults have associated complications. The classic triad of intermittent abdominal pain, jaundice, and a right upper quadrant abdominal mass is found only in minority of patients.
In infants, choledochal cysts usually lead to obstruction of the bile ducts and retention of bile. This leads to jaundice and an enlarged liver. If the obstruction is not relieved, permanent damage may occur to the liver - scarring and cirrhosis - with the signs of portal hypertension (obstruction to the flow of blood through the liver) and ascites (fluid accumulation in the abdomen). There is an increased risk of cancer in the wall of the cyst.
In older individuals, choledochal cysts are more likely to cause abdominal pain and intermittent episodes of jaundice and occasionally cholangitis (inflammation within the bile ducts caused by the spread of bacteria from the intestine into the bile ducts). Pancreatitis also may occur. The cause of these complications may be related to either abnormal flow of bile within the ducts or the presence of gallstones
Diagnosis
Direct hyperbilirubinemia
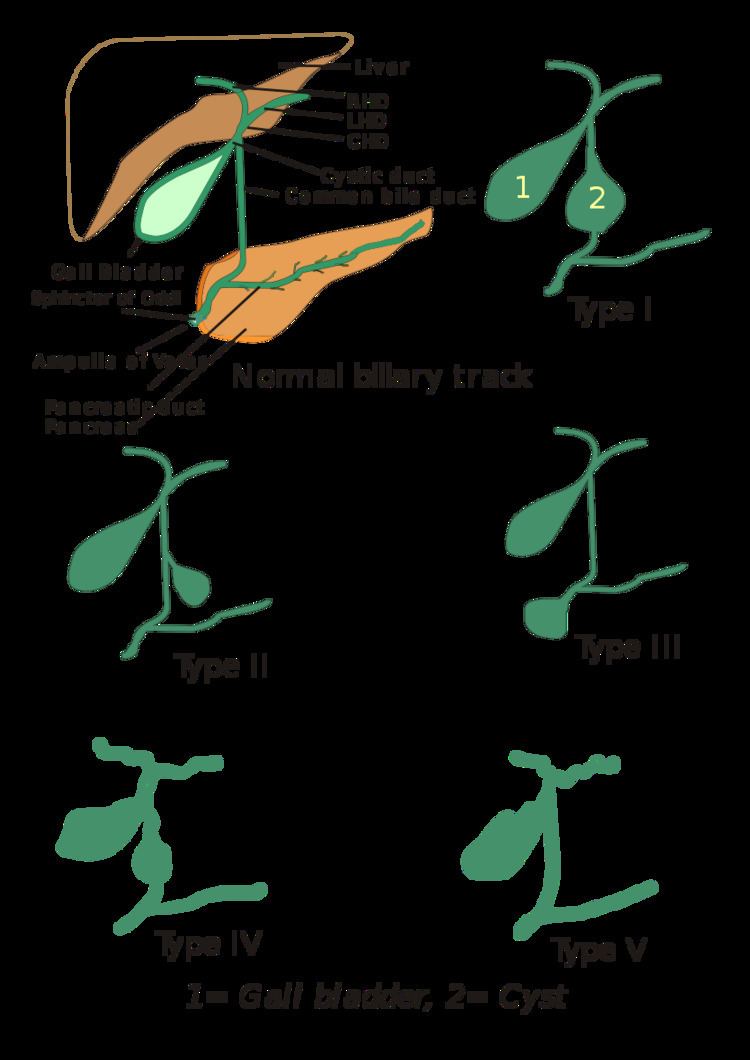
Types
They were classified into 5 types by Todani in 1977.
Classification was based on site of the cyst or dilatation. Type I to IV has been subtyped.
Treatment
Choledochal cysts are treated by surgical excision of the cyst with the formation of a roux-en-Y anastomosis to the biliary duct.
Future complications include cholangitis and a 2% risk of malignancy, which may develop in any part of the biliary tree. A recent article published in Journal of Surgery suggested that choledochal cysts could also be treated with single-incision laparoscopic hepaticojejunostomy with comparable results and less scarring. In cases of saccular type of cyst, excision and placement of T-shaped tube is done.
Currently, there is no accepted indication for fetal intervention in the management of prenatally suspected choledochal cysts.