
Entrez 1493 | Human Mouse Ensembl ENSG00000163599 | |
Aliases CTLA4, ALPS5, CD, CD152, CELIAC3, CTLA-4, GRD4, GSE, IDDM12, cytotoxic T-lymphocyte associated protein 4 External IDs Similar S100A10, ICAM 1, Uteroglobin | ||
Ctla 4 the unwanted player in cancer
CTLA4 or CTLA-4 (cytotoxic T-lymphocyte-associated protein 4), also known as CD152 (cluster of differentiation 152), is a protein receptor that, functioning as an immune checkpoint, downregulates immune responses. CTLA4 is constitutively expressed in Tregs but only upregulated in conventional T cells after activation. It acts as an "off" switch when bound to CD80 or CD86 on the surface of antigen-presenting cells.
Contents
- Ctla 4 the unwanted player in cancer
- Function
- Structure
- Clinical significance
- Germline haploinsufficiency
- Clinical and laboratory manifestations
- Treatment
- Agonists to reduce immune activity
- Antagonists to increase immune activity
- Interactions
- References
The CTLA-4 protein is encoded by the Ctla4 gene in mice and the CTLA4 gene in humans.
Function
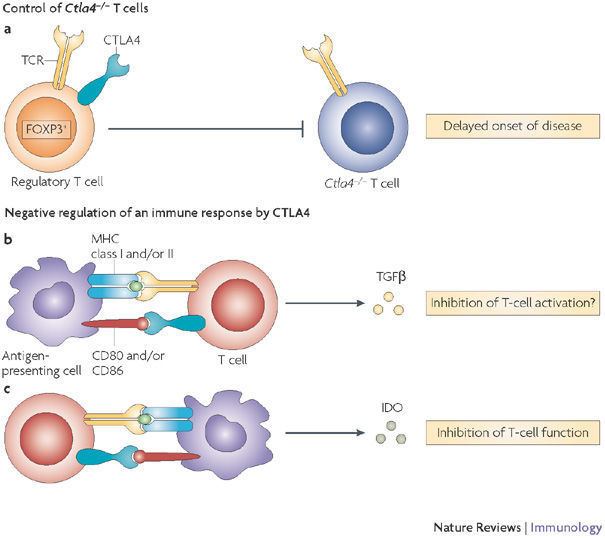
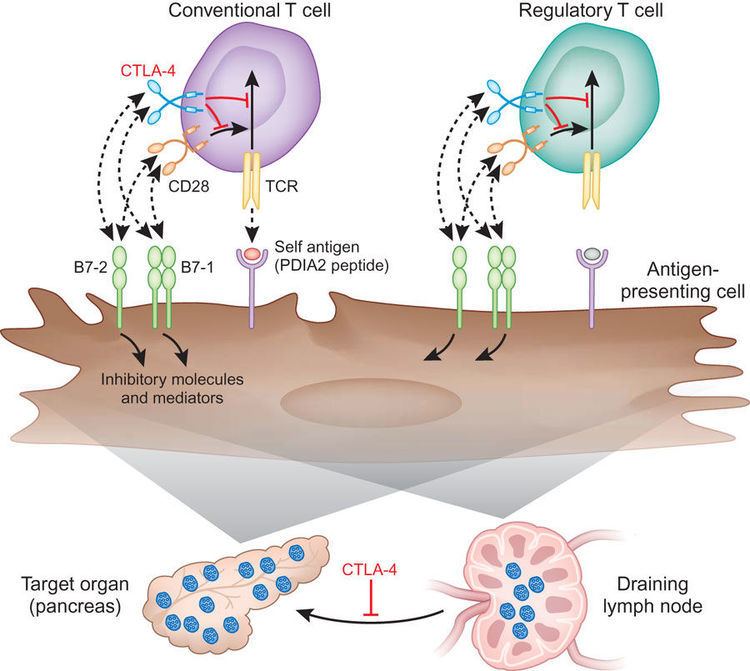
CTLA4 is a member of the immunoglobulin superfamily that is expressed by activated T cells and transmits an inhibitory signal to T cells. CTLA4 is homologous to the T-cell co-stimulatory protein, CD28, and both molecules bind to CD80 and CD86, also called B7-1 and B7-2 respectively, on antigen-presenting cells. CTLA-4 binds CD80 and CD86 with greater affinity and avidity than CD28 thus enabling it to outcompete CD28 for its ligands. CTLA4 transmits an inhibitory signal to T cells, whereas CD28 transmits a stimulatory signal. CTLA4 is also found in regulatory T cells and contributes to its inhibitory function. T cell activation through the T cell receptor and CD28 leads to increased expression of CTLA-4.
The mechanism by which CTLA-4 acts in T cells remains somewhat controversial. Biochemical evidence suggested that CTLA-4 recruited a phosphatase to the T cell receptor, thus attenuating the signal. This work remains unconfirmed in the literature since its first publication. More recent work has suggested that CTLA-4 may function in vivo by capturing and removing B7-1 and B7-2 from the membranes of antigen-presenting cells, thus making these unavailable for triggering of CD28.
In addition to that, it has been found, DC-Treg interaction causes sequestration of Fascin-1, an actin-bundling protein essential for immunological synapse formation, and skews Fascin-1–dependent actin polarization in antigen presenting dendritic cells toward the T reg cell adhesion zone. Although it is reversible upon T regulatory cell disengagement, this sequestration of essential cytoskeletal components causes a lethargic state of dendritic cells, leading to reduced T cell priming. This suggests Treg-mediated immune suppression is a multi-step process. In addition to CTLA-4 CD80/CD86 interaction, fascin dependent polarization of cytoskeleton towards DC-Treg immune synapse play a pivotal role.
CTLA-4 may also function via modulation of cell motility and/or signaling through PI3 kinase Early multiphoton microscopy studies observing T-cell motility in intact lymph nodes appeared to give evidence for the so-called ‘reverse-stop signaling model’. In this model CTLA-4 reverses the TCR-induced ‘stop signal’ needed for firm contact between T cells and antigen-presenting cells (APCs). However, those studies compared CTLA-4 positive cells, which are predominantly regulatory cells and are at least partially activated, with CTLA-4 negative naive T cells. The disparity of these cells in multiple regards may explain some of these results. Other groups who have analyzed the effect of antibodies to CTLA-4 in vivo have concluded little or no effect upon motility. Antibodies to CTLA-4 may exert additional effects when used in vivo, by binding and thereby depleting regulatory T cells.
Structure
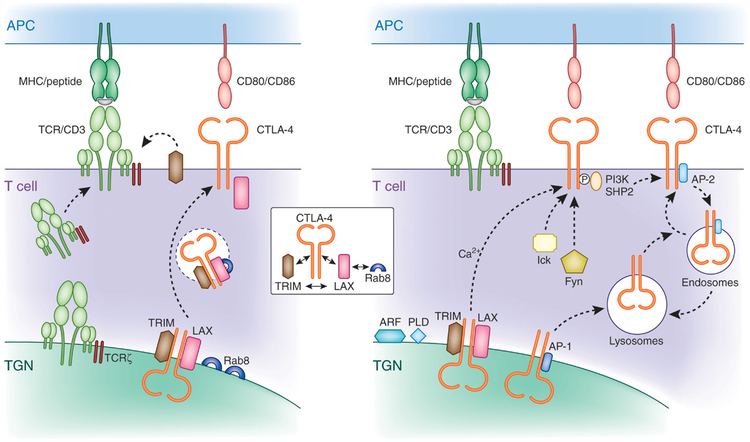
The protein contains an extracellular V domain, a transmembrane domain, and a cytoplasmic tail. Alternate splice variants, encoding different isoforms, have been characterized. The membrane-bound isoform functions as a homodimer interconnected by a disulfide bond, while the soluble isoform functions as a monomer. The intracellular domain is similar to that of CD28, in that it has no intrinsic catalytic activity and contains one YVKM motif able to bind PI3K, PP2A and SHP-2 and one proline-rich motif able to bind SH3 containing proteins. The first role of CTLA-4 in inhibiting T cell responses seem to be directly via SHP-2 and PP2A dephosphorylation of TCR-proximal signalling proteins such as CD3 and LAT. CTLA-4 can also affect signalling indirectly via competing with CD28 for CD80/86 binding. CTLA-4 can also bind PI3K, although the importance and results of this interaction are uncertain.
Clinical significance
Variants in this gene have been associated with insulin-dependent diabetes mellitus, Graves' disease, Hashimoto's thyroiditis, celiac disease, systemic lupus erythematosus, thyroid-associated orbitopathy, primary biliary cirrhosis and other autoimmune diseases.
Polymorphisms of the CTLA-4 gene are associated with autoimmune diseases such as autoimmune thyroid disease and multiple sclerosis, though this association is often weak. In Systemic Lupus Erythematosus (SLE), the splice variant sCTLA-4 is found to be aberrantly produced and found in the serum of patients with active SLE.
Germline haploinsufficiency
Germline haploinsufficiency of CTLA4 leads to CTLA4 deficiency or CHAI disease (CTLA4 haploinsufficiency with autoimmune infiltration), a rare genetic disorder of the immune system. This may cause a dysregulation of the immune system and may result in lymphoproliferation, autoimmunity, hypogammaglobulinemia, recurrent infections, and may slightly increase one’s risk of lymphoma. CTLA4 mutations have first been described by a collaboration between the groups of Dr. Gulbu Uzel, Dr. Steven Holland, and Dr. Michael Lenardo from the National Institute of Allergy and Infectious Disease, Dr. Thomas Fleisher from the NIH Clinical Center at the National Institutes of Health, and their collaborators in 2014. In the same year a collaboration between the groups of Dr. Bodo Grimbacher, Dr. Shimon Sakaguchi, Dr. Lucy Walker and Dr. David Sansom and their collaborators described a similar phenotype.
CTLA4 mutations are inherited in an autosomal dominant manner. This means a person only needs one abnormal gene from one parent. The one normal copy is not enough to compensate for the one abnormal copy. Dominant inheritance means most families with CTLA4 mutations have affected relatives in each generation on the side of the family with the mutation.
Clinical and laboratory manifestations
Symptomatic patients with CTLA4 mutations are characterized by an immune dysregulation syndrome including extensive T cell infiltration in a number of organs, including the gut, lungs, bone marrow, central nervous system, and kidneys. Most patients have diarrhea or enteropathy. Lymphadenopathy and hepatosplenomegaly are also common, as is autoimmunity. The organs affected by autoimmunity vary but include thrombocytopenia, hemolytic anemia, thyroiditis, type I diabetes, psoriasis, and arthritis. Respiratory infections are also common. Importantly, the clinical presentations and disease courses are variable with some individuals severely affected, whereas others show little manifestation of disease. This “variable expressivity,” even within the same family, can be striking and may be explained by differences in lifestyle, exposure to pathogens, treatment efficacy, or other genetic modifiers. This condition is described to have incomplete Penetrance of disease. Penetrance is said to be incomplete when some individuals fail to express the trait and seem completely asymptomatic, even though they carry the allele. The penetrance is estimated to be about 60%.
The clinical symptoms are caused by abnormalities of the immune system. Most patients develop reduced levels of at least one immunoglobulin isotype, and have low CTLA4 protein expression in T regulatory cells, hyperactivation of effector T cells, low switched memory B cells, and progressive loss of circulating B cells.
Treatment
Once a diagnosis is made, the treatment is based on an individual’s clinical condition and may include standard management for autoimmunity and immunoglobulin deficiencies. A recent study treated a Korean CHAI disease patient with CTLA4 mimetic, CTLA4-Ig (e.g.. abatacept) and was able to control immune activity and improve patient symptoms. Regular administration of abatacept improved the patient’s severe anemia and diarrhea (3L/day) and brought 3-year-long hospitalization to an end.
Agonists to reduce immune activity
The comparatively higher binding affinity of CTLA4 has made it a potential therapy for autoimmune diseases. Fusion proteins of CTLA4 and antibodies (CTLA4-Ig) have been used in clinical trials for rheumatoid arthritis. The fusion protein CTLA4-Ig is commercially available as Orencia (abatacept). A second generation form of CTLA4-Ig known as belatacept was recently approved by the FDA based on favorable results from the randomized Phase III BENEFIT (Belatacept Evaluation of Nephroprotection and Efficacy as First Line Immunosuppression Trial) study. It was approved for renal transplantation in patients that are sensitized to Epstein–Barr virus (EBV).
Antagonists to increase immune activity
Conversely, there is increasing interest in the possible therapeutic benefits of blocking CTLA4 (using antagonistic antibodies against CTLA such as ipilimumab (FDA approved for melanoma in 2011) as a means of inhibiting immune system tolerance to tumours and thereby providing a potentially useful immunotherapy strategy for patients with cancer. This is the first approved immune checkpoint blockade therapy. Another (not yet approved) is tremelimumab.
Interactions
CTLA-4 has been shown to interact with: