
Pronunciation /θəˈlɪdəmaɪd/ MedlinePlus a699032 Molar mass 258.23 g/mol Bioavailability 90% | AHFS/Drugs.com Monograph Formula C13H10N2O4 CAS ID 50-35-1 | |
 | ||
Trade names Thalomid, Immunoprin, Talidex, Talizer, Neurosedyn (S) Pregnancycategory AU: X (High risk)US: X (Contraindicated) IUPAC ID (RS)-2-(2,6-dioxopiperidin-3-yl)-1H-isoindole-1,3(2H)-dione | ||
Thalidomide, sold under the brand name Immunoprin, among others, is an immunomodulatory drug and the prototype of the thalidomide class of drugs. Today, thalidomide is used mainly as a treatment of certain cancers (multiple myeloma) and of a complication of leprosy.
Contents
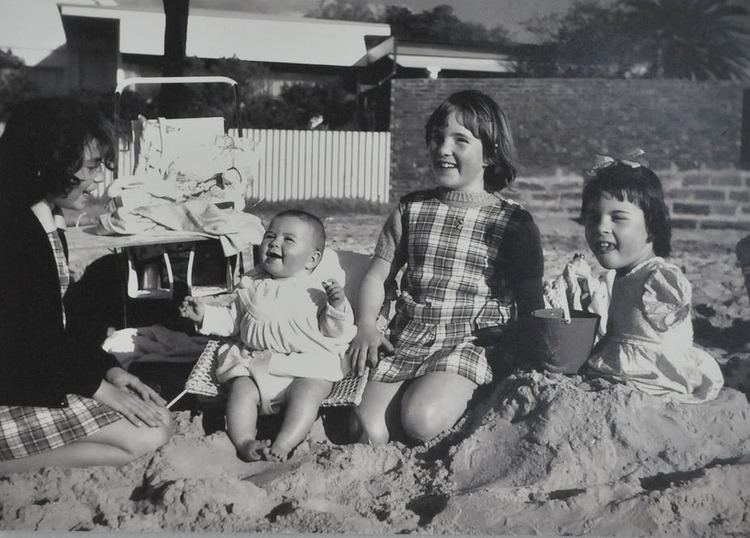
- Surviving thalidomide
- Medical uses
- Adverse effects
- Carcinogenicity
- Contraindications
- Interactions
- Overdose
- Mechanism of action
- Cereblon CRBN
- Other actions
- History
- Leprosy treatment
- Cancer treatment
- Thalidomide analogs
- Regulatory approved uses
- Birth defects crisis
- Aftermath of scandal
- Germany
- United Kingdom
- Australia
- Canada
- United States
- Notable cases
- Change in drug regulations
- Research
- References

Thalidomide was first marketed in 1957 in West Germany under the trade-name Contergan. The German drug company Chemie Grünenthal developed and sold the drug. Primarily prescribed as a sedative or hypnotic, thalidomide also claimed to cure "anxiety, insomnia, gastritis, and tension". Afterwards, it was used against nausea and to alleviate morning sickness in pregnant women. Thalidomide became an over-the-counter drug in West Germany on October 1, 1957. Shortly after the drug was sold in West Germany, between 5,000 and 7,000 infants were born with phocomelia (malformation of the limbs). Only 40% of these children survived. Throughout the world, about 10,000 cases were reported of infants with phocomelia due to thalidomide; only 50% of the 10,000 survived. Those subjected to thalidomide while in the womb experienced limb deficiencies in a way that the long limbs either were not developed or presented themselves as stumps. Other effects included deformed eyes and hearts, deformed alimentary and urinary tracts, blindness and deafness. The negative effects of thalidomide led to the development of more structured drug regulations and control over drug use and development.

Surviving thalidomide
Medical uses
Thalidomide is used for a number of conditions including erythema nodosum leprosum, multiple myeloma (in combination with dexamethasone), and various other cancers, for some symptoms of HIV/AIDS, Crohn's disease, sarcoidosis, graft-versus-host disease, rheumatoid arthritis, Behçet's disease and a number of skin conditions that have not responded to usual treatment.

The bacterium that causes tuberculosis is related to leprosy. Thalidomide may be helpful in some cases where standard TB drugs and corticosteroids are not sufficient to resolve severe inflammation in the brain.
There is no conclusive evidence that thalidomide or lenalidomide is useful to bring about or maintain remission in Crohn's disease.
Adverse effects
Thalidomide may cause side effects, such as polyneuropathy, fatigue, skin rash, and venous thromboembolism (VTE), or blood clots, which could lead to stroke or myocardial infarction.
Adverse effects by frequency:
Very common (may affect more than 1 in 10 people):
Common (may affect up to 1 in 10 people):
Uncommon (may affect up to 1 in 100 people):
Rare (may affect up to 1 in 1,000 people):
Very rare (may affect up to 1 in 10,000 people):

† Peripheral neuropathy may be irreversible and usually results from chronic (usually a matter of months) exposure to thalidomide.
Carcinogenicity

Animal studies did not demonstrate any carcinogenicity even when rats and mice were exposed to up to 11 times the therapeutic dose of thalidomide. Despite this there have been some concerns that it may cause secondary malignancies in patients with multiple myeloma. The FDA has issued a statement that it is investigating these concerns.

Some clinical trials have supported this claim and the major secondary malignancy that thalidomide is associated with is acute myeloid leukaemia. The MHRA of the UK and Health Canada of Canada have also issued warnings to healthcare professionals regarding the risk of secondary malignancies due to thalidomide exposure.
Contraindications
Contraindications include:

Interactions
There are no expected pharmacokinetic interactions between thalidomide and other medicines due to its neutral effects on p-glycoprotein and P450 cytochromes. It may interact with sedatives due to its sedative action. It may also interact with bradycardic agents due to its bradycardia-inducing effects. The risk of peripheral neuropathy may be increased by concomitant treatment with other agents known to cause peripheral neuropathy. The risk of venous thromboembolisms with thalidomide seems to be increased when patients are treated with oral contraceptives or other cytotoxic agents (including doxorubicin and melphalan) concurrently. Thalidomide may interfere with the contraceptive effects of various contraceptives and hence it is advised that women of reproductive age use at least two different means of contraception to ensure that no child will be conceived while they are receiving thalidomide.
Overdose
Eighteen cases of overdoses have been reported to date with doses of up to 14.4 g without any reported fatalities. No specific antidote for overdoses exists and treatment is purely supportive.
Mechanism of action
The precise mechanism of action for thalidomide is unknown, but possible mechanisms include anti-angiogenic and oxidative stress-inducing effects. It also inhibits TNF-α, IL-6, IL-10 and IL-12 production, modulates the production of IFN-γ and enhances the production of IL-2, IL-4 and IL-5 by immune cells. It increases lymphocyte count, costimulates T cells and modulates natural killer cell cytotoxicity. It also inhibits NF-κB and COX-2 activity.
In 1990, a group of researchers in Brazil noted that TNF alpha levels went up in leprosy reactional states and observed that TNF levels decreased in some patients on treatment with thalidomide, hence potentially explaining the efficacy of thalidomide in treating ENL.
The mechanism of thalidomide's teratogenic action has led to over 2000 research papers and the proposal of 15 or 16 plausible mechanisms. Angiogenesis is critical during limb development of the foetus. Thalidomide can directly inhibit angiogenesis induced by bFGF or VEGF in vivo. Teratogenic analogs inhibit angiogenesis whereas nonteratogenic analogs do not inhibit angiogenesis. In 2009, research by other groups confirmed "conclusively that loss of newly formed blood vessels is the primary cause of thalidomide teratogenesis, and developing limbs are particularly susceptible because of their relatively immature, highly angiogenic vessel network".
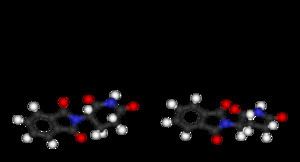
Thalidomide is racemic; the individual enantiomers can racemize due to the acidic hydrogen at the chiral centre, which is the carbon of the glutarimide ring bonded to the phthalimide substituent. The racemization process can occur in vivo so that any plan to administer a purified single enantiomer to avoid the teratogenic effects will most likely be in vain.
Cereblon (CRBN)
Several studies have now shown that the mechanism of action for thalidomide involves binding to the protein cereblon, a ubiquitin ligase substrate adapter protein, which is important in limb formation and the proliferative capacity of myeloma cells. Ubiquitin ligases function by reducing the cellular levels of proteins and thalidomide has been shown to alter the set of proteins which CRBN can degrade. Cereblon's relevance to human congenital defects was confirmed in studies that reduced the production of cereblon in developing chick and zebrafish embryos using genetic techniques. These embryos had defects similar to those treated with thalidomide. Interestingly, mice treated with thalidomide do not display teratogenicity of their offspring as seen in humans.
Other actions
Thalidomide binds to and acts as an antagonist of the androgen receptor (AR). In accordance, it can produce gynecomastia and sexual dysfunction as side effects in men. DIMP is a non-steroidal antiandrogen which was one of the first antiandrogens to be developed, and is structurally related to thalidomide.
History
Thalidomide was developed by German pharmaceutical company Chemie Grünenthal (now Grünenthal GmbH). After obtaining a twenty-year patent in April 1954, Chemie Grünenthal started clinical trials and as early as November 1956 marketed thalidomide for the treatment of respiratory infections under the trade name Grippex, a combination drug that contained thalidomide, quinine, vitamin C, phenacetin and acetylsalicylic-acid (aspirin).
Researchers at Chemie Grünenthal also found that thalidomide was a particularly effective antiemetic that had an inhibitory effect on morning sickness. Hence, on October 1, 1957, the company launched thalidomide and began aggressively marketing it under the trade name Contergan. It was proclaimed a "wonder drug" for insomnia, coughs, colds and headaches.
During this time period, the use of medications during pregnancy was not strictly controlled, and drugs were not thoroughly tested for potential harm to the fetus. Thousands of pregnant women took the drug to relieve their symptoms. At the time of the drug's development, scientists did not believe any drug taken by a pregnant woman could pass across the placental barrier and harm the developing fetus, even though the effect of alcohol on fetal development had been documented by case studies on alcoholic mothers since at least 1957. There soon appeared reports of findings of abnormalities in children being born, traced back to the use of the drug thalidomide. In late 1959, it was noticed that peripheral neuritis developed in patients who took the drug over a period of time, and it was only after this point that thalidomide ceased to be provided over the counter.
Hence, while initially considered safe, the drug was responsible for teratogenic deformities in children born after their mothers used it during pregnancies, prior to the third trimester. In November 1961, thalidomide was taken off the market due to massive pressure from the press and public. Experts estimate that the drug thalidomide led to the death of approximately 2,000 children and serious birth defects in more than 10,000 children, about 5,000 of them in West Germany. The regulatory authorities in East Germany did not approve thalidomide. One reason for the initially unobserved side effects of the drug and the subsequent approval in West Germany was that at that time drugs did not have to be tested for teratogenic effects. They had been tested on rodents only, as was usual at the time.
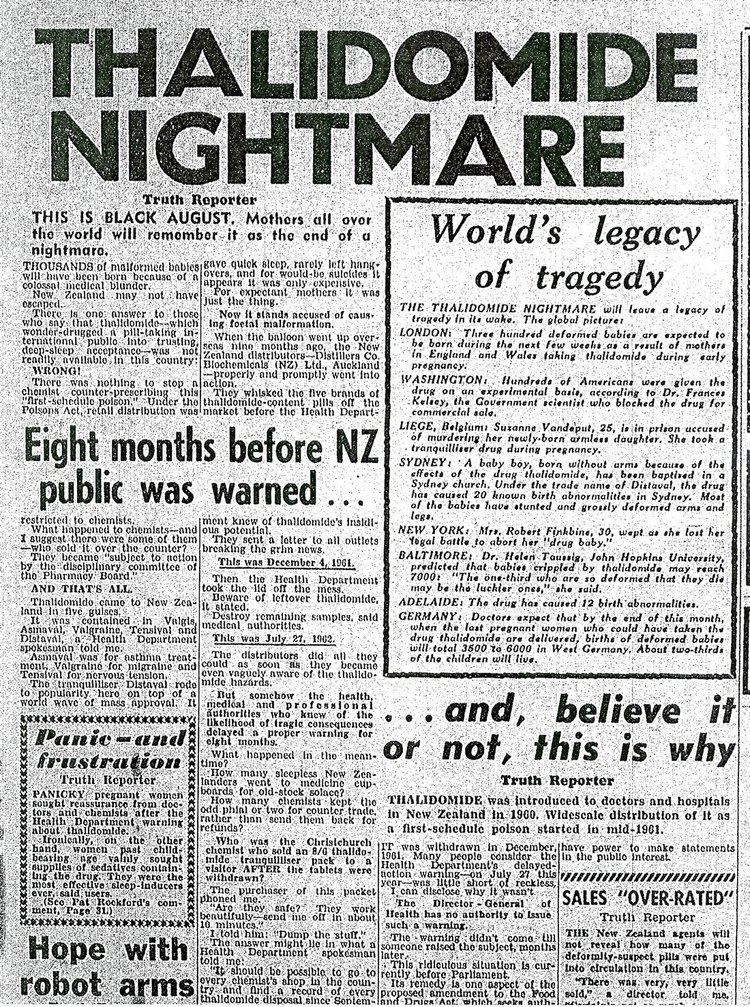
In the UK, the British pharmaceutical company The Distillers Company (Biochemicals) Ltd, a subsidiary of Distillers Co. Ltd. (now part of Diageo plc), marketed thalidomide under the brand name Distaval as a remedy for morning sickness throughout the United Kingdom, Australia and New Zealand. Their advertisement claimed that "Distaval can be given with complete safety to pregnant women and nursing mothers without adverse effect on mother or child...Outstandingly safe Distaval has been prescribed for nearly three years in this country." Around the world, more and more pharmaceutical companies started to produce and market the drug under license from Chemie Grünenthal. By the mid 1950s, 14 pharmaceutical companies were marketing thalidomide in 46 countries under 37 (some reports suggest 51) different trade names.
In the U.S., representatives from Chemie Grünenthal approached Smith, Kline & French (SKF), now GlaxoSmithKline (GSK) with a request to market and distribute the drug in North America. A memorandum rediscovered in 2010 in the archives of the U.S. Food and Drug Administration (FDA) shows that, as part of its in-licensing approach, Smith, Kline and French conducted animal tests and ran a clinical trial of the drug in the United States involving 875 people, including pregnant women, in 1956–57. In 1956, researchers at SKF involved in clinical trials noted that even when used in very high doses, thalidomide could not induce sleep in mice. And when administered at doses 50 to 650 times larger than that claimed by Chemie Grünenthal to be "sleep inducing", the researchers could still not achieve the hypnotic effect in animals that it had on humans. After completion of the trial, and based on reasons kept hidden for decades, SKF declined to commercialize the drug. Later, Chemie Grünenthal, in 1958, reached an agreement with William S Merrell Company in Cincinnati, Ohio, (later Richardson-Merrell, now part of Sanofi), to market and distribute thalidomide throughout the United States.
The U.S. FDA refused to approve thalidomide for marketing and distribution. However, the drug was distributed in large quantities for testing purposes, after the American distributor and manufacturer Richardson-Merrell had applied for its approval in September 1960. The official in charge of the FDA review, Frances Oldham Kelsey, did not rely on information from the company, which did not include any test results. Richardson-Merrell was called on to perform tests and report the results. The company demanded approval six times, and was refused each time. Nevertheless, a total of 17 children with thalidomide-induced malformations were born in the U.S.
In Canada, the history of the drug thalidomide dates back to April 1, 1961. There were many different forms sold, with the most common variant being Talimol. Two months after Talimol went on sale, pharmaceutical companies sent physicians letters warning about the risk of birth defects. It was not until March 2, 1962, that both drugs were banned from the Canadian market by the FDD, and soon afterward physicians were warned to destroy their supplies.
Leprosy treatment
In 1964, Israeli physician Jacob Sheskin administered thalidomide to a patient critically ill with leprosy. The patient exhibited erythema nodosum leprosum (ENL), a painful skin condition, one of the complications of leprosy. This was attempted despite the ban on thalidomide's use, but results were favourable: the patient slept for hours and was able to get out of bed without aid upon awakening. A clinical trial studying the use of thalidomide in leprosy soon followed.
Thalidomide has been used by Brazilian physicians as the drug of choice for the treatment of severe ENL since 1965, and by 1996, at least 33 cases of thalidomide embryopathy were recorded in people born in Brazil after 1965. Since 1994, the production, dispensing, and prescription of thalidomide have been strictly controlled, requiring women to use two forms of birth control and submit to regular pregnancy tests. Despite this, cases of thalidomide embryopathy continue, with at least 100 cases identified in Brazil between 2005 and 2010. 5.8 million thalidomide pills were distributed throughout Brazil in this time period, largely to poor Brazilians in areas with poor access to healthcare, and these cases have occurred despite the controls.
In 1998 the FDA approved the drug's use in the treatment of ENL. Because of thalidomide's potential for causing birth defects, the drug may be distributed only under tightly controlled conditions. The FDA required that Celgene Corporation, which planned to market thalidomide under the brand name Thalomid, establish a system for thalidomide education and prescribing safety (STEPS) oversight program. The conditions required under the program include limiting prescription and dispensing rights to authorized prescribers and pharmacies only, keeping a registry of all patients prescribed thalidomide, providing extensive patient education about the risks associated with the drug, and providing periodic pregnancy tests for women who take the drug.
In 2010, the World Health Organisation (WHO) stated that it did not recommend thalidomide due the difficulty of adequately controlling its use, and due to the availability of clofazimine.
Cancer treatment
Shortly after the teratogenic properties of thalidomide were recognized in the mid-1960s, its anti-cancer potential was explored and two clinical trials were conducted in people with advanced cancer, including some people with multiple myeloma; the trials were inconclusive.
Little further work was done with thalidomide in cancer until the 1990s.
Judah Folkman pioneered studies into the role of angiogenesis (the proliferation and growth of blood vessels) in the development of cancer, and in the early 1970s had shown that solid tumors could not expand without it. In 1993 he surprised the scientific world by hypothesizing the same was true of blood cancers, and the next year he published work showing that a biomarker of angiogenesis was higher in all people with cancer, but especially high in people with blood cancers, and other evidence emerged as well. Meanwhile, a member of his lab, Robert D'Amato, was looking for angiogenesis inhibitors, and discovered in 1994 that thalidomide inhibited angiogenesis. Around that time, the wife of a man who was dying of multiple myeloma and whom standard treatments had failed, called Folkman asking him about his anti-angiogenesis ideas. Folkman convinced the patient's doctor to try thalidomide, and that doctor conducted a clinical trial of thalidomide for people with multiple myeloma in which about a third of the subjects responded to the treatment. The results of that trial were published in the New England Journal of Medicine in 1999.
After further work was done by Celgene and others, in 2006 the U.S. Food and Drug Administration granted accelerated approval for thalidomide in combination with dexamethasone for the treatment of newly diagnosed multiple myeloma patients.
Thalidomide analogs
The exploration of the antiangiogenic and immunomodulatory activities of thalidomide has led to the study and creation of thalidomide analogs. Celgene has sponsored numerous clinical trials with analogues to thalidomide, such as lenalidomide, that are substantially more powerful and have fewer side effects — except for greater myelosuppression. In 2005, Celgene received FDA approval for lenalidomide (Revlimid) as the first commercially useful derivative. Revlimid is available only in a restricted distribution setting to avoid its use during pregnancy. Further studies are being conducted to find safer compounds with useful qualities. Another more potent analog, pomalidomide, is now FDA approved. Additionally, apremilast was approved by the FDA in March 2014. These thalidomide analogs can be used to treat different diseases, or used in a regimen to fight two conditions.
Interest turned to pomalidomide, a derivative of thalidomide marketed by Celgene. It is a very active anti-angiogenic agent and also acts as an immunomodulator. Pomalidomide was approved in February 2013 by the U.S. Food and Drug Administration (FDA) as a treatment for relapsed and refractory multiple myeloma. It received a similar approval from the European Commission in August 2013, and is expected to be marketed in Europe under the brand name Imnovid.
Regulatory approved uses
+ : designated Orphan drug under the Orphan Drug Act of 1983
Birth defects crisis
In the late 1950s and early 1960s, more than 10,000 children in 46 countries were born with deformities such as phocomelia as a consequence of thalidomide use. The severity and location of the deformities depended on how many days into the pregnancy the mother was; thalidomide taken on the 20th day of pregnancy caused central brain damage, day 21 would damage the eyes, day 22 the ears and face, day 24 the arms, and leg damage would occur if taken up to day 28. Thalidomide did not damage the foetus if taken after 42 days gestation.
It is not known exactly how many worldwide victims of the drug there have been, although estimates range from 10,000 to 20,000 to 100,000. Despite the side effects, thalidomide was sold in pharmacies in Canada until 1962.
In the United Kingdom, the drug was licensed in 1958 and withdrawn in 1961. Of the approximately 2,000 babies born with defects, around half died within a few months and 466 survived to at least 2010.
In Spain, thalidomide was widely available throughout the 1970s, perhaps even into the 1980s. There were two reasons for this. First, state controls and safeguarding were poor; indeed, it was not until 2008 that the government even admitted the country had ever imported thalidomide. Second, Grünenthal failed to insist that its sister company in Madrid warn Spanish doctors, and permitted it to not warn them. The Spanish advocacy group for victims of thalidomide estimates that in 2015, there were 250–300 living victims of thalidomide in Spain.
The Australian obstetrician William McBride and the German paediatrician Widukind Lenz suspected a link between birth defects and the drug, a theory Lenz proved in 1961. McBride was later awarded a number of honors, including a medal and prize money by L'Institut de la Vie in Paris. Further animal tests were conducted by Dr George Somers, Chief Pharmacologist of Distillers Company in Britain, which showed foetal abnormalities in rabbits. Similar results were also published showing these effects in rats and other species.
In East Germany, the head of the central pharmacy control commission, Friedrich Jung, suspected an antivitaminic effect of thalidomide as derivative of glutamic acid. Meanwhile, in West Germany, it took some time before the increase in dysmelia at the end of the 1950s was connected with thalidomide. In 1958 Karl Beck, a former pediatric doctor in Bayreuth wrote an article in a local newspaper claiming a relationship between nuclear weapons testing and cases of dysmelia in children. Based on this, FDP whip Erich Mende requested an official statement from the federal government. For statistical reasons, the main data series used to research dysmelia cases started by chance at the same time as the approval date for thalidomide. After the Nazi regime with its Law for the Prevention of Hereditarily Diseased Offspring used mandatory statistical monitoring to commit various crimes, western Germany had been very reluctant to monitor congenital disorders in a similarly strict way. The parliamentary report rejected any relation with radioactivity and the abnormal increase of dysmelia. Also the DFG research project installed after the Mende request was not helpful. The project was led by pathologist Franz Büchner who ran the project to propagate his teratological theory. Büchner saw lack of healthy nutrition and behavior of the mothers as being more important than genetic reasons. Furthermore, it took a while to install a Surgeon General in Germany; the Federal Ministry of Health (Germany) was not founded until 1962, some months after thalidomide was banned from the market. In Germany approximately 2,500 thalidomide babies were born.
Several countries either restricted the drug's use or never approved it. Ingeborg Eichler, a member of the Austrian pharmaceutical admission conference, enforced thalidomide (tradename Softenon) being sold under the rules of prescription medication and as a result relatively few affected children were born in Austria and Switzerland. In the United States, pharmacologist Frances Oldham Kelsey M.D. withstood pressure from the Richardson-Merrell company and refused Food and Drug Administration (FDA) approval to market thalidomide, saying further studies were needed. This reduced the impact of thalidomide in United States patients. Although thalidomide was never approved for sale in the United States at the time, millions of tablets had been distributed to physicians during a clinical testing program. It was impossible to know how many pregnant women had been given the drug to help alleviate morning sickness or as a sedative.
Aftermath of scandal
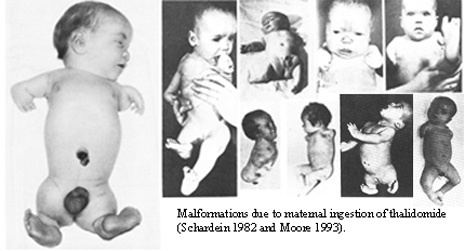
The numerous reports of malformations in babies brought about the awareness of the side effects of the drug on pregnant women. The birth defects caused by the drug thalidomide can range from moderate malformation to more severe forms. Possible birth defects include phocomelia, dysmelia, amelia, bone hypoplasticity, and other congenital defects affecting the ear, heart, or internal organs. Franks et al. looked at how the drug affected newborn babies, the severity of their deformities, and reviewed the drug in its early years. Webb in 1963 also reviewed the history of the drug and the different forms of birth defects it had caused. "The most common form of birth defects from thalidomide is shortened limbs, with the arms being more frequently affected. This syndrome is the presence of deformities of the long bones of the limbs resulting in shortening and other abnormalities."
Germany
In 1968, a large criminal trial began in Germany, charging several Grünenthal officials with negligent homicide and injury. After Grünenthal settled with the victims in April 1970, the trial ended in December 1970 with no finding of guilt. As part of the settlement, Grünenthal paid 100 million DM into a special foundation; the German government added 320 million DM. The foundation paid victims a one-time sum of 2,500-25,000 DM (depending on severity of disability) and a monthly stipend of 100-450 DM. The monthly stipends have since been raised substantially and are now paid entirely by the government (as the foundation had run out of money). Grünenthal paid another 50 million Euros into the foundation in 2008.
On 31 August 2012, Grünenthal chief executive Harald F. Stock, PhD, who served as the Chief Executive Officer of Grünenthal GmbH from January 2009 to May 28, 2013 and was also a Member of Executive Board until May 28, 2013, apologized for the first time for producing the drug and remaining silent about the birth defects. At a ceremony, Stock unveiled a statue of a disabled child to symbolize those harmed by thalidomide and apologized for not trying to reach out to victims for over 50 years. At the time of the apology, there were 5,000 to 6,000 sufferers still alive. Victim advocates called the apology "insulting" and "too little, too late", and criticized the company for not compensating victims. They also criticized the company for their claim that no one could have known the harm the drug caused, arguing that there were plenty of red flags at the time.
United Kingdom
In 1968, after a long campaign by The Sunday Times, a compensation settlement for the UK victims was reached with Distillers Company (now part of Diageo), which had distributed the drug in the UK. This compensation, which is distributed by the Thalidomide Trust in the UK, was substantially increased by Diageo in 2005. The UK Government gave survivors a grant of £20 million, to be distributed through the Thalidomide Trust, in December 2009.
Australia
Melbourne woman Lynette Rowe, who was born without limbs, led an Australian class action lawsuit against the drug's manufacturer, Grünenthal, which fought to have the case heard in Germany. The Supreme Court of Victoria dismissed Grünenthal's application in 2012, and the case was heard in Australia. On 17 July 2012, Rowe was awarded an out-of-court settlement, believed to be in the millions of dollars and paving the way for class action victims to receive further compensation. In February 2014, the Supreme Court of Victoria endorsed the settlement of $89 million AUD to 107 victims of the drug in Australia and New Zealand.
Canada
The drug thalidomide's birth defects in children affected many people's lives, and from these events came the formation of the group called The Thalidomide Victims Association of Canada, a group of 120 Canadian survivors. Their goal was to prevent future usage of drugs that could be of potential harm to mothers and babies. The members from the thalidomide victims association were involved in the STEPS program, which aimed to prevent teratogenicity.
The effects of thalidomide increased fears regarding the safety of pharmaceutical drugs. The Society of Toxicology of Canada was formed after the effects of thalidomide were made public, focusing on toxicology as a discipline separate from pharmacology. The need for the testing and approval of the toxins in certain pharmaceutical drugs became more important after the disaster. The Society of Toxicology of Canada is responsible for the Conservation Environment Protection Act, focusing on researching the impact to human health of chemical substances. Thalidomide brought on changes in the way drugs are tested, what type of drugs are used during pregnancy, and increased the awareness of potential side effects of drugs.
According to Canadian news magazine program W5, most, but not all, victims of thalidomide receive annual benefits as compensation from the Government of Canada. Excluded are those who cannot provide the documentation the government requires.
United States
For correctly denying the application despite the pressure from Richardson-Merrell, Kelsey eventually received the President's Award for Distinguished Federal Civilian Service at a 1962 ceremony with President John F. Kennedy. In September 2010, the FDA honored Kelsey with the first Kelsey award. The award, given annually to an FDA staff member, came 50 years after Kelsey, then a new medical officer at the agency, first reviewed the application from the William S. Merrell Company of Cincinnati. Cardiologist Helen B. Taussig learned of the damaging effects of the drug thalidomide on newborns and in 1967, testified before Congress on this matter after a trip to Germany where she worked with infants with phocomelia (severe limb deformities). As a result of her efforts, thalidomide was banned in the United States and Europe.
Notable cases
Change in drug regulations
The disaster prompted many countries to introduce tougher rules for the testing and licensing of drugs, such as the Kefauver Harris Amendment (U.S.), Directive 65/65/EEC1 (E.U.), and the Medicines Act 1968. In the United States, the new regulations strengthened the FDA, among other ways, by requiring applicants to prove efficacy and to disclose all side-effects encountered in testing. The FDA subsequently initiated the Drug Efficacy Study Implementation to reclassify drugs already on the market.
Research
Investigational uses include: