
ICD-O 9080 eMedicine med/3449 | ICD-10 C62.9 (ILDS C62.930) DiseasesDB 3604 1295212966 MeSH D013724 | |
 | ||
A teratoma is a tumor with tissue or organ components resembling normal derivatives of more than one germ layer. Although the teratoma may be monodermal or polydermal (originating from one or more germ layers), its cells may differentiate in ways suggesting other germ layers. The tissues of a teratoma, although normal in themselves, may be quite different from surrounding tissues and may be highly disparate; teratomas have been reported to contain hair, teeth, bone and, very rarely, more complex organs or processes such as brain matter, eyes, torso, and hands, feet, or other limbs.
Contents
- Terminology
- Signs and symptoms
- Complications
- Pathophysiology
- Hypotheses of origin
- Mature teratoma
- Dermoid cyst
- Fetus in fetu and fetiform teratoma
- Struma ovarii
- Diagnosis
- Classification
- Malignant transformation
- Extraspinal ependymoma
- Surgery
- Chemotherapy
- Follow up
- Epidemiology
- Research
- Other animals
- References
Usually, a teratoma will contain no organs but rather one or more tissues normally found in organs such as the brain, thyroid, liver, and lung. Sometimes, the teratoma has within its capsule one or more fluid-filled cysts; when a large cyst occurs, there is a potential for the teratoma to produce a structure within the cyst that resembles a fetus. Because they are encapsulated, teratomas are usually benign, although several forms of malignant teratoma are known and some of these are common forms of teratoma. A mature teratoma is typically benign and found more commonly in women, while an immature teratoma is typically malignant and is more often found in men.
Teratomas are thought to be present at birth (congenital), but small ones often remain undiscovered until much later in life.
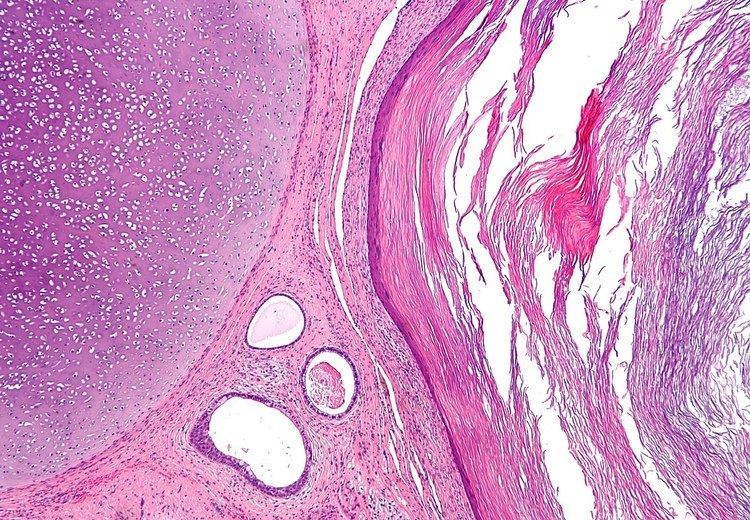
Definitive medical diagnosis of a teratoma is based on its histology.
Terminology
As is true throughout oncology (the study of tumors, malignant and benign), the nomenclature for these tumors continually evolves on the basis of threads of consensus in the scientific literature regarding the tumors' classification (which is based on shared embryologic origins, clinicopathologic characteristics, and so on). As science advances, more is understood about how one can differentiate tumors that formerly seemed alike. For example, the scientific knowledge of tumor markers, genomics, and proteomics regularly advances. In this environment, tumor names may slip over the years between synonymity, hyponymy and hypernymy, and deprecation. Some terms that have been synonymous with teratoma include dysembryoma, teratoblastoma, organoid tumor, and teratoid tumor.
The words "teratoma" and "mature teratoma" both have been used to refer to a benign growth, while the word "teratoma" may also refer to "immature teratoma", a cancerous growth. Avoiding misunderstanding due to such polysemy is part of why tumor nomenclature changes over decades. The nomenclatural changes are voluntary, based on scientists agreeing or debating in the literature regarding what to call particular neoplastic entities (types of tumors).
The term "malignant teratoma" has sometimes been used as a synonym for nonseminomatous germ cell tumor.
Signs and symptoms
Teratomas of germ cell origin usually are found (i.e., present) in adult men and women, but they may also be found in children and infants. Teratomas of embryonal origin are most often found in babies at birth, in young children, and, since the advent of ultrasound imaging, in fetuses.
The most commonly diagnosed fetal teratomas are sacrococcygeal teratoma (Altman types I, II, and III) and cervical (neck) teratoma. Because these teratomas project from the fetal body into the surrounding amniotic fluid, they can be seen during routine prenatal ultrasound exams. Teratomas within the fetal body are less easily seen with ultrasound; for these, MRI of the pregnant uterus is more informative.
Complications
Teratomas are not dangerous for the fetus unless there is either a mass effect or a large amount of blood flow through the tumor (known as vascular steal). The mass effect frequently consists of obstruction of normal passage of fluids from surrounding organs. The vascular steal can place a strain on the growing heart of the fetus, even resulting in heart failure, and thus must be monitored by fetal echocardiography.
After surgery, there is a risk of regrowth in place, or in nearby organs.
Pathophysiology
Teratomas belong to a class of tumors known as nonseminomatous germ cell tumor (N.S.G.C.T.). All tumors of this class are the result of abnormal development of pluripotent cells: germ cells and embryonal cells. Teratomas of embryonic origin are congenital; teratomas of germ cell origin may or may not be congenital (this is not known). The kind of pluripotent cell appears to be unimportant, apart from constraining the location of the teratoma in the body.
Teratomas derived from germ cells occur in the testes in men and ovaries in women. Teratomas derived from embryonic cells usually occur on the subject's midline: in the brain, elsewhere in the skull, in the nose, in the tongue, under the tongue, and in the neck (cervical teratoma), mediastinum, retroperitoneum, and attached to the coccyx. Teratomas may also occur elsewhere: very rarely in solid organs (most notably the heart and liver) and hollow organs (such as the stomach and bladder), and more commonly on the skull sutures.
Hypotheses of origin
Concerning the origin of teratomas, there exist numerous hypotheses. These hypotheses are not to be confused with the unrelated hypothesis that fetus in fetu (see below) is not a teratoma at all but rather a parasitic twin.
Mature teratoma
A mature teratoma is a grade 0 teratoma. Mature teratomas are highly variable in form and histology, and may be solid, cystic, or a combination of solid and cystic. A mature teratoma often contains several different types of tissue such as skin, muscle, and bone. Skin may surround a cyst and grow abundant hair (see Dermoid cyst). Mature teratomas generally are benign; malignant mature teratomas are of several distinct types.
Dermoid cyst
A dermoid cyst is a mature cystic teratoma containing hair (sometimes very abundant) and other structures characteristic of normal skin and other tissues derived from the ectoderm. The term is most often applied to teratoma on the skull sutures and in the ovaries of females.
Fetus in fetu and fetiform teratoma
Fetus in fetu and fetiform teratoma are rare forms of mature teratoma that include one or more components resembling a malformed fetus. Both forms may contain or appear to contain complete organ systems, even major body parts such as torso or limbs. Fetus in fetu differs from fetiform teratoma in having an apparent spine and bilateral symmetry.
Most authorities agree that fetiform teratomas are highly developed mature teratomas; the natural history of fetus in fetu is controversial. There also may be a cultural difference, with fetiform teratoma being reported more often in ovarian teratomas (by gynecologists) and fetus in fetu being reported more often in retroperitoneal teratomas (by general surgeons). Fetus in fetu has often been interpreted as a fetus growing within its twin. As such, this interpretation assumes a special complication of twinning, one of several grouped under the term parasitic twin. In this regard, it is noteworthy that in many cases the fetus in fetu is reported to occupy a fluid-filled cyst within a mature teratoma. Cysts within mature teratoma may have partially developed organ systems; reports include cases of partial cranial bones, long bones and a rudimentary beating heart.
Regardless of whether fetus in fetu and fetiform teratoma are one entity or two, they are distinct from and not to be confused with ectopic pregnancy.
Struma ovarii
A struma ovarii (literally: goitre of the ovary) is a rare form of mature teratoma that contains mostly thyroid tissue.
Diagnosis
Teratomas are thought to originate in utero, and therefore can be considered congenital tumors. Many teratomas are not diagnosed until much later in childhood or in adulthood. Large tumors are more likely to be diagnosed early on. Sacrococcygeal and cervical teratomas are often detected by prenatal ultrasound. Additional diagnostic methods may include prenatal MRI. In rare circumstances, the tumor is so large that the fetus may be damaged or die. In the case of large sacrococcygeal teratomas, a significant portion of the fetus' blood flow is redirected toward the teratoma (a phenomenon called steal syndrome), causing heart failure, or hydrops, of the fetus. In certain cases, fetal surgery may be indicated.
Beyond the newborn period, symptoms of a teratoma depend on its location and organ of origin. Ovarian teratomas often present with abdominal or pelvic pain, caused by torsion of the ovary or irritation of its ligaments. A recently discovered condition where ovarian teratomas cause encephalitis associated with antibodies against the N-methyl-D-aspartate receptor (NMDAR) - often simply referred to as "Anti-NMDA receptor encephalitis", was identified as a serious complication. Patients develop a multistage illness that progresses from psychosis, memory deficits, seizures, and language disintegration into a state of unresponsiveness with catatonic features often associated with abnormal movements, and autonomic and breathing instability. Testicular teratomas present as a palpable mass in the testis; mediastinal teratomas often cause compression of the lungs or the airways and may present with chest pain and/or respiratory symptoms.
Some teratomas contain yolk sac elements, which secrete alpha-fetoprotein (AFP). Detection of AFP may help to confirm the diagnosis and is often used as a marker for recurrence or treatment efficacy, but is rarely the method of initial diagnosis. (Maternal serum alpha-fetoprotein, or MSAFP, is a useful screening test for other fetal conditions, including Down syndrome, spina bifida and abdominal wall defects such as gastroschisis.)
Classification
Regardless of location in the body, a teratoma is classified according to a cancer staging system. This indicates whether chemotherapy or radiation therapy may be needed in addition to surgery. Teratomas commonly are classified using the Gonzalez-Crussi grading system: 0 or mature (benign); 1 or immature, probably benign; 2 or immature, possibly malignant (cancerous); and 3 or frankly malignant. If frankly malignant, the tumor is a cancer for which additional cancer staging applies.
Teratomas are also classified by their content: a solid teratoma contains only tissues (perhaps including more complex structures); a cystic teratoma contains only pockets of fluid or semi-fluid such as cerebrospinal fluid, sebum, or fat; a mixed teratoma contains both solid and cystic parts. Cystic teratomas usually are grade 0 and, conversely, grade 0 teratomas usually are cystic.
Grade 0, 1 and 2 pure teratomas have the potential to become malignant (grade 3), and malignant pure teratomas have the potential to metastasize. These rare forms of teratoma with malignant transformation may contain elements of somatic (non germ cell) malignancy such as leukemia, carcinoma or sarcoma. A teratoma may contain elements of other germ cell tumors, in which case it is not a pure teratoma but rather is a mixed germ cell tumor and is malignant. In infants and young children, these elements usually are endodermal sinus tumor, followed by choriocarcinoma. Finally, a teratoma can be pure and not malignant yet highly aggressive: this is exemplified by growing teratoma syndrome, in which chemotherapy eliminates the malignant elements of a mixed tumor, leaving pure teratoma which paradoxically begins to grow very rapidly.
Malignant transformation
A "benign" grade 0 (mature) teratoma nonetheless has a risk of malignancy. Recurrence with malignant endodermal sinus tumor has been reported in cases of formerly benign mature teratoma, even in fetiform teratoma and fetus in fetu. Squamous cell carcinoma has been found in a mature cystic teratoma at the time of initial surgery.
A grade 1 immature teratoma that appears to be benign (e.g., because AFP is not elevated) has a much higher risk of malignancy, and requires adequate follow-up. This grade of teratoma also may be difficult to diagnose correctly. It can be confused with other small round cell neoplasms such as neuroblastoma, small cell carcinoma of hypercalcemic type, primitive neuroectodermal tumor, Wilm's tumor, desmoplastic small round cell tumor, and non-Hodgkin lymphoma.
A teratoma with malignant transformation (TMT) is a very rare form of teratoma that may contain elements of somatic (non germ cell) malignant tumors such as leukemia, carcinoma or sarcoma. Of 641 children with pure teratoma, nine developed TMT: five carcinoma, two glioma, and two embryonal carcinoma (here, these last are classified among germ cell tumors).
Extraspinal ependymoma
Extraspinal ependymoma, usually considered to be a glioma (a type of non-germ cell tumor), may be an unusual form of mature teratoma.
Surgery
The treatment of choice is complete surgical removal (i.e., complete resection). Teratomas are normally well-encapsulated and non-invasive of surrounding tissues, hence they are relatively easy to resect from surrounding tissues. Exceptions include teratomas in the brain, and very large, complex teratomas that have pushed into and become interlaced with adjacent muscles and other structures.
Prevention of recurrence does not require en bloc resection of surrounding tissues.
Chemotherapy
For malignant teratomas, usually, surgery is followed by chemotherapy.
Teratomas that are in surgically inaccessible locations, or are very complex, or are likely to be malignant (due to late discovery and/or treatment) sometimes are treated first with chemotherapy.
Follow-up
Although often described as benign, a teratoma does have malignant potential. In a UK study of 351 infants and children diagnosed with "benign" teratoma reported 227 with MT, 124 with IT. Five years after surgery, event-free survival was 92.2% and 85.9%, respectively, and overall survival was 99% and 95.1%. A similar study in Italy reported on 183 infants and children diagnosed with teratoma. At 10 years after surgery, event free and overall survival were 90.4% and 98%, respectively.
Depending on which tissue(s) it contains, a teratoma may secrete a variety of chemicals with systemic effects. Some teratomas secrete the "pregnancy hormone" human chorionic gonadotropin (βhCG), which can be used in clinical practice to monitor the successful treatment or relapse in patients with a known HCG-secreting teratoma. This hormone is not recommended as a diagnostic marker, because most teratomas do not secrete it. Some teratomas secrete thyroxine, in some cases to such a degree that it can lead to clinical hyperthyroidism in the patient. Of special concern is the secretion of alpha-fetoprotein (AFP); under some circumstances AFP can be used as a diagnostic marker specific for the presence of yolk sac cells within the teratoma. These cells can develop into a frankly malignant tumor known as yolk sac tumor or endodermal sinus tumor.
Adequate follow-up requires close observation, involving repeated physical examination, scanning (ultrasound, MRI, or CT), and measurement of AFP and/or βhCG.
Epidemiology
Embryonal teratomas most commonly occur in the sacrococcygeal region: sacrococcygeal teratoma is the single most common tumor found in newly born humans.
Of teratomas on the skull sutures, approximately 50% are found in or adjacent to the orbit. Limbal dermoid is a choristoma, not a teratoma.
Teratoma qualifies as a rare disease, but is not extremely rare. Sacrococcygeal teratoma alone is diagnosed at birth in one out of 40,000 humans. Given the current human population and birth-rate, this equals five per day or 1800 per year. Add to that number sacrococcygeal teratomas diagnosed later in life, and teratomas in other locales, and the incidence approaches ten thousand new diagnoses of teratoma per year.
Research
In light of the ethical issues surrounding the source of human stem cells, teratomas are being looked at as an alternative source for research because they lack the potential to grow into functional human beings.
Other animals
Ovarian teratomas have been reported in mares, mountain lions, and in canines. Teratomas also occur, rarely, in other species.