
ICD-9-CM 75.36 | ||
 | ||
Fetal surgery is any of a broad range of surgical techniques that are used to treat birth defects in fetuses who are still in the pregnant uterus.
Contents
- Technique
- Safety and complications
- Indications
- Research
- Minimally invasive fetal surgery
- History
- References
Technique
Tocolytics are generally given to prevent labor; however, these should be given if the risk is higher for the fetus inside the womb than if delivered, such as may be the case in intrauterine infection, unexplained vaginal bleeding and fetal distress. An H2 antagonist is usually given for anaesthesia the evening before and the morning of the operation, and an antacid is usually given before induction to reduce the risk of acid aspiration. Rapid sequence induction is often used for sedation and intubation.
Open fetal surgery is similar in many respects to a normal cesarean section performed under general anesthesia, except that the fetus remains dependent on the placenta and is returned to the uterus. A hysterotomy is performed on the pregnant woman, and once the uterus is open and the fetus is exposed, the fetal surgery begins. Typically, this surgery consists of an interim procedure intended to allow the fetus to remain in utero until it has matured enough to survive delivery and neonatal surgical procedures.
Upon completion of the fetal surgery, the fetus is put back inside the uterus and the uterus and abdominal wall are closed up. Before the last stitch is made in the uterine wall, the amniotic fluid is replaced. The mother remains in the hospital for 3–7 days for monitoring. Often babies who have been operated on in this manner are born pre-term.
Safety and complications
The main priority is maternal safety, and, secondary, avoiding preterm labor and achieving the aims of the surgery. Open fetal surgery is possible first after approximately 18 weeks of gestation due to fetal size and fragility before that, and up to approximately 30 weeks of gestation due to increased risk of premature labor and, practically, the preference for delivering the child and performing the surgery ex utero instead. The risk of premature labor is increased by concomitant risk factors such as multiple gestation, a history of maternal smoking, and very young or old maternal age.
Open fetal surgery has proven to be reasonably safe for the mother. For the fetus, safety and effectiveness are variable, and depend on the specific procedure, the reasons for the procedure, and the gestational age and condition of the fetus. The overall perinatal mortality after open surgery has been estimated to be approximately 6%, according to a study in the United States 2003.
All future pregnancies for the mother require cesarean delivery because of the hysterotomy. However, there is no presented data suggesting decreased fertility for the mother.
Indications
Prenatal repair of neural tube defects such as myelomeningocele (spina bifida cystica) is a growing option in the United States. Although the procedure is technically challenging, children treated with open fetal repair have significantly improved outcomes compared to children whose defects are repaired shortly after birth. Specifically, fetal repair reduces the rate of ventriculoperitoneal shunt dependence and Chiari malformation, while improving motor skills at 30 months of age compared to post-natal repair. Children having fetal repair are twice as likely to walk independently at 30 months of age than children undergoing post-natal repair. As a result, open fetal repair of spina bifida is now considered standard of care at fetal specialty centers.
Other conditions that potentially are treated by open fetal surgery include:
Research
Ganogen Research Institute CEO Dr. Eugene Gu has proposed transplanting the human fetal heart into patients with hypoplastic left heart syndrome or other severe congenital heart defects in utero. He has also proposed transplanting the human fetal kidney into patients with bilateral renal agenesis. This would represent a significant advance in the field of fetal surgery if successful. Gu has already shown that human fetal hearts and kidneys can be transplanted into immunocompromised rats where they subsequently show growth and function.
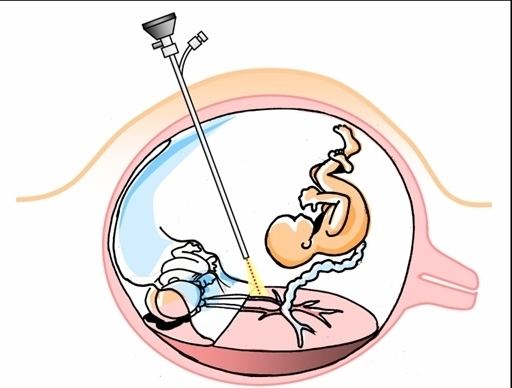
Minimally invasive fetal surgery
Minimally-invasive fetoscopic surgery (akin to 'keyhole surgery'has proven to be very useful for some, but not all, fetal conditions.
History
Fetal surgical techniques using animal models were first developed at the University of California, San Francisco in 1980 by Dr. Michael R. Harrison and his research colleagues, including Dr. Diana L. Farmer.
On April 26, 1981, the first human open fetal surgery in the world was performed at University of California, San Francisco under the direction of Dr. Michael Harrison. The fetus in question had a congenital hydronephrosis, a blockage in the urinary tract that caused the kidney to dangerously extend. To correct this a vesicostomy was performed placing a catheter in the fetus allowing the urine to be released normally. The blockage itself was removed surgically after birth.
Further advances have been made in the years since this first operation. New techniques have allowed additional defects to be treated and for less invasive forms of fetal surgical intervention.
The first two percutaneous ultrasound-guided fetal balloon valvuloplasties, a type of fetal surgery for severe aortic valve obstruction in the heart, were reported in 1991. Among the first dozen reported attempts at this repair in the 1990s, only two children survived long-term.