
Genus Staphylococcus Rank Species | Phylum Firmicutes Higher classification Staphylococcus | |
 | ||
Scientific name Staphylococcus haemolyticus Similar Bacteria, Staphylococcus hominis, Staphylococcus warneri, Staphylococcus capitis, Staphylococcus lugdunensis | ||
Staphylococcus haemolyticus is a member of the coagulase-negative staphylococci (CoNS). It is part of the skin flora of humans, and its largest populations are usually found at the axillae, perineum, and inguinal areas. S. haemolyticus also colonizes primates and domestic animals. It is a well-known opportunistic pathogen, and is the second-most frequently isolated CoNS (S. epidermidis is the first). Infections can be localized or systemic, and are often associated with the insertion of medical devices. The highly antibiotic-resistant phenotype and ability to form biofilms make S. haemolyticus a difficult pathogen to treat.
Contents
Biology and biochemistry
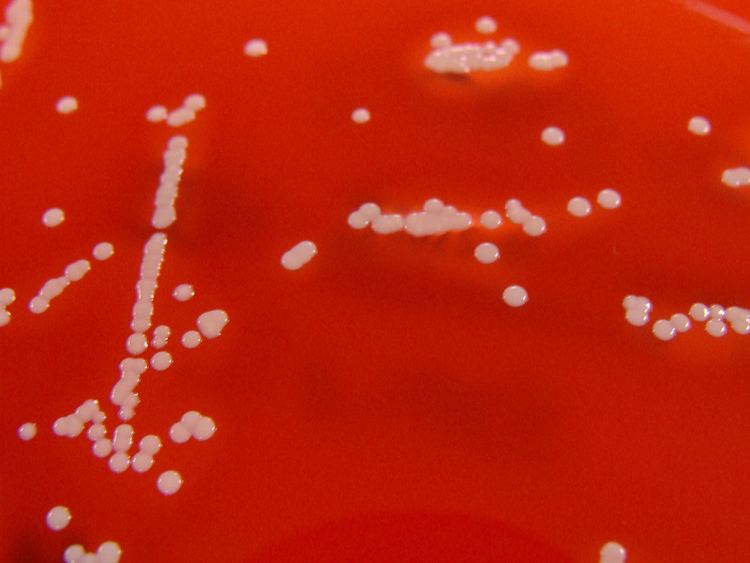
S. haemolyticus is nonmotile, nonsporulating, facultatively anaerobic, and Gram-positive. Cells are typically coccus-shaped and range from 0.8-1.3 μm in diameter. It lives on a wide variety of substrates, including glucose, glycerol, maltose, sucrose, and trehalose. It also tests positive for acetoin production, arginine, dihydrolase, benzidine, catalase, hemolysis, and lipase; it tests negative for coagulase, DNase, ornithine decarboxylase, phosphatase, urease, and oxidase.
Growth conditions
Optimal growth occurs between 30 and 40 °C in the presence of oxygen and 10% NaCl. However, some strains can grow at temperatures that range between 18 and 45 °C. Growth at 15 °C or 15% NaCl is poor or absent.
Genome structure
The S. haemolyticus strain JCSC1435 genome contains a 2,685,015 bp chromosome and three plasmids of 2,300 bp, 2,366 bp, and 8,180 bp. The chromosome is comparable in size to those of S. aureus and S. epidermidis and contains a similar G+C content. In addition, a large proportion of the open reading frames (ORFs) are conserved across all three species. On average, orthologous ORFs are 78% identical. However, S. haemolyticus does have unique chromosome regions distributed near oriC (the origin of chromosomal DNA replication), and these regions are collectively referred to as the “oriC environ”.
As noted, some S. haemolyticus ORFs differ from S. aureus and S. epidermidis. Some of these ORFs encode gene products with known biological features, such as the regulation of RNA synthesis, the transport of ribose and ribitol, and the essential components of nucleic acid and cell wall teichoic acid biosynthesis. Other unique ORFs likely encode products involved with bacterial pathogenesis and at least three of these ORFs show homology to staphylococcal hemolysins.
The S. haemolyticus genome also contains many insertion sequences (ISs). These IS elements may promote frequent genomic rearrangements which accelerate the diversification of the species. Theoretically, these adaptations might help S. haemolyticus overcome the adverse effects of chemical exposure (i.e. the use of antibiotics). The table below contains a list of genes known to be associated with S. haemolyticus antibiotic resistance.
Cell wall
Like other Gram-positive microbes, S. haemolyticus has a thick, rather homogenous, cell wall (60-80 nm) composed of peptidoglycan, teichoic acid, and protein. Peptidoglycan of group A3 (with L-lysine as the diamino acid in position 3 of the peptide subunit and a glycine-rich interpeptide bridge) is a characteristic feature of this microbe, and the two predominant cross-bridges are COOH-Gly-Gly-Ser-Gly-Gly-NH2 and COOH-Ala-Gly-Ser-Gly-Gly-NH2. Alterations of these cross-bridges are implicated in glycopeptide resistance. S. haemolyticus teichoic acids are water-soluble polymers with repeating phosphodiester groups covalently linked to peptidoglycan. Peptidoglycan type L-Lys-Gly 3.5-4.0, L-Ser0.9-1.5 Teichoic acid contains both glycerol and N-acetylglucosamine. The major cell wall fatty acids are CBr-15, CBr-17, C18, and C20.
Capsule
Certain strains of S. haemolyticus are capable of producing a capsular polysaccharide (CP). S. haemolyticus strain JCSC1435 contains a capsule operon located within the “oriC environ”. This operon contains 13 ORFs in a 14,652-bp region and is referred to as the capsh locus. The first seven genes of capsh (capAsh through capGsh) are homologous to the S. aureus cap5 or cap8 locus. However, capH through capM are unique to S. haemolyticus, and this region encodes enzymes for a unique trideoxy sugar residue that is N-acylated by aspartic acid.
CP production is influenced by culture medium and growth phase. Cultivation in tryptic soy broth (TSB)], TSB with 1% glucose, brain heart infusion broth, or Columbia broth with 2% NaCl favors the production of CP; cultivation on Columbia salt agar plates is suboptimal. Only trace amounts of CP are generated before the end of exponential phase, and the maximal rate of CP production does not occur until early stationary phase.
CP is considered a virulence factor because it provides resistance against complement-mediated polymorphonuclear neutrophil phagocytosis.
Biofilm formation
The ability to adhere to medical devices and subsequently form biofilms is a major virulence factor associated with S. haemolyticus. Biofilm formation increases antibiotic resistance and often leads to persistent infections. S. haemolyticus biofilms are not polysaccharide intercellular adhesin (PIA) dependent, and the lack of the ica operon (the gene cluster that encodes the production of PIA) can be used to distinguish S. haemolyticus isolates from other CoNS species.
Biofilm formation is influenced by a variety of factors including carbohydrates, proteins, and extracellular DNA. Detachment assays with NaIO4, proteinase K, or DNase result in 38%, 98%, and 100% detachment, respectively. The high level of detachment associated with DNase treatment has led several authors to suggest a cell-to-surface and/or cell-to-cell adhesion function for extracellular DNA. Biofilm formation also appears to be influenced by the presence of glucose and NaCl. Biofilm formation is enhanced when cultivated in TSB with 1% glucose and decreased when cultivated in TSB with 3% NaCl. The production of a capsular polysaccharide decreases biofilm formation.
Subinhibitory concentrations (subminimum inhibitory concentrations) of the antibiotic dicloxacillin also affect the growth of S. haemolyticus biofilms. Biofilms formed in the presence of subinhibitory concentrations of dicloxacillin contain less biomass and have an altered composition. They are thinner, cover less surface area, and are less hydrophobic, but they also have an increased level of resistance to dicloxacillin.
Toxins
Some S. haemolyticus strains produce enterotoxins (SE) and/or hemolysins. In a study of 64 S. haemolyticus strains, production of SEA, SEB, SEC, and/or SEE was noted (only SED was absent). In addition, 31.3% of the strains were found to produce at least one type of enterotoxin.
Identification
S. haemolyticus can be identified on the species level using a variety of manual and automated methods. The most frequently employed are: the reference method (based on growth tests), API ID 32 Staph (bioMe´rieux), Staph-Zym (Rosco), UZA (a rapid 4-h method), and polymerase chain reaction and electrophoretic analysis of the 16S rRNA, hsp60, or sodA gene sequence. Preference towards a particular method usually depends on convenience, economics, and required specificity (some species have identical 16S rRNA).
Clinical importance
S. haemolyticus is the second-most clinically isolated CoNS (S. epidermidis is the first) and it is considered an important nosocomial pathogen. Human infections include: native valve endocarditis, septicemia, peritonitis, and urinary tract, wound, bone, and joint infections. Infrequent soft-tissue infections usually occur in immunocompromised patients. Like other CoNS, S. haemolyticus is often associated with the insertion of foreign bodies, such as prosthetic valves, cerebrospinal fluid shunts, orthopedic prostheses, and intravascular, urinary, and dialysis catheters. S. haemolyticus is multi-drug resistant and able to form biofilms, which makes infections especially difficult to treat.
Vascular catheter-associated infections
S. haemolyticus can colonize central venous catheters and cause serious medical complications. Colonization occurs when S. haemolyticus migrates from the skin, along the external surface of the device, or from the hub, due to manipulation by health care workers. In either scenario, a high probability exists that the microbe will form a biofilm. These infections can remain localized or become systemic (i.e. bacteremia). The severity of infection varies depending on the type of catheter, frequency of manipulation, and virulence factors of the S. haemolyticus strain. Removal of the catheter is usually considered to be the best treatment, but this is not always possible. Alternatively, vancomycin or teicoplanin may be administered. Recent evidence suggests that glycopeptides can be supplemented with β-lactams to work synergistically.
Antibiotic resistance
S. haemolyticus has the highest level of antibiotic resistance among the CoNS. Various strains are resistant to one or more of these antibiotics: penicillins, cephalosporins, macrolides, quinolones, tetracyclines, aminoglycosides, glycopeptides, and fosfomycin (see table in Genome structure), and multidrug resistance is common. As indicated above, even glycopeptide-resistant (vancomycin and teicoplanin) strains have begun to emerge. Meropenem would be suitable for treatment.