
Specialty gynaecology ICD-9-CM 615.9 MedlinePlus 001484 | ICD-10 N71 DiseasesDB 4283 eMedicine med/676 ped/678 | |
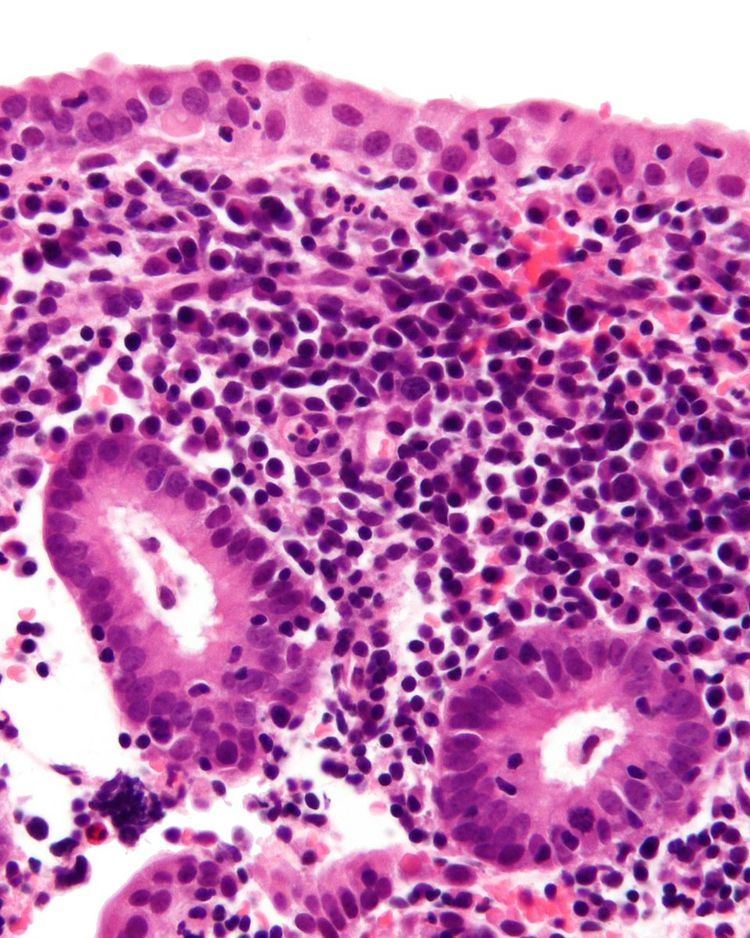 | ||
Endometritis is inflammation of the endometrium, the inner lining of the uterus.
Contents
Pathologists have traditionally classified endometritis as either acute or chronic: acute endometritis is characterized by the presence of microabscesses or neutrophils within the endometrial glands, while chronic endometritis is distinguished by variable numbers of plasma cells within the endometrial stroma. The most common cause of endometritis is infection. Symptoms include lower abdominal pain, fever and abnormal vaginal bleeding or discharge. Caesarean section, prolonged rupture of membranes and long labor with multiple vaginal examinations are important risk factors. Treatment is usually with broad-spectrum antibiotics.
The term "endomyometritis" is sometimes used to specify inflammation of the endometrium and the myometrium.
Acute endometritis
Acute Endometritis is characterized by infection. The organisms most often isolated are believed to be because of compromised abortions, delivery, medical instrumentation, and retention of placental fragments. There is not enough evidence for the use of prophylactic antibiotics to prevent endometritis after manual removal of placental in vaginal birth. Histologically, neutrophilic infiltration of the endometrial tissue is present during acute endometritis. The clinical presentation is typically high fever and purulent vaginal discharge. Menstruation after acute endometritis is excessive and in uncomplicated cases can resolve after 2 weeks of clindamycin and gentamicin IV antibiotic treatment.
In certain populations, it has been associated with Mycoplasma genitalium and pelvic inflammatory disease.
Chronic endometritis
Chronic Endometritis is characterized by the presence of plasma cells in the stroma. Lymphocytes, eosinophils, and even lymphoid follicles may be seen, but in the absence of plasma cells, are not enough to warrant a histologic diagnosis. It may be seen in up to 10% of all endometrial biopsies performed for irregular bleeding. The most common organisms are Chlamydia trachomatis (chlamydia), Neisseria gonorrhoeae (gonorrhea), Streptococcus agalactiae (Group B Streptococcus), Mycoplasma hominis, tuberculosis, and various viruses. Most of these agents are capable of causing chronic pelvic inflammatory disease (PID). Patients suffering from chronic endometritis may have an underlying cancer of the cervix or endometrium (although infectious etiology is more common). Antibiotic therapy is curative in most cases (depending on underlying etiology), with fairly rapid alleviation of symptoms after only 2 to 3 days.
Chronic granulomatous endometritis is usually caused by tuberculous. The granulomas are small, sparse, and without caseation. The granulomas take up to 2 weeks to develop and since the endometrium is shed every 4 weeks, the granulomas are poorly formed.
In human medicine, pyometra (also a veterinary condition of significance) is regarded as a form of chronic endometritis seen in elderly women causing stenosis of the cervical os and accumulation of discharges and infection. Symptom in chronic endometritis is blood stained discharge but in pyometra the patient complaints of lower abdominal pain.
Pyometra
Pyometra describes an accumulation of pus in the uterine cavity. In order for pyometra to develop, there must be both an infection and blockage of cervix. Signs and symptoms include lower abdominal pain (suprapubic), rigors, fever, and the discharge of pus on introduction of a sound into the uterus. Pyometra is treated with antibiotics, according to culture and sensitivity.