
Rank Species | Phylum Chlamydiae Higher classification Chlamydia | |
 | ||
Similar Bacteria, Neisseria, Chlamydiae, Chlamydophila psittaci, Haemophilus | ||
Time lapse video of the chlamydia trachomatis developmental cycle
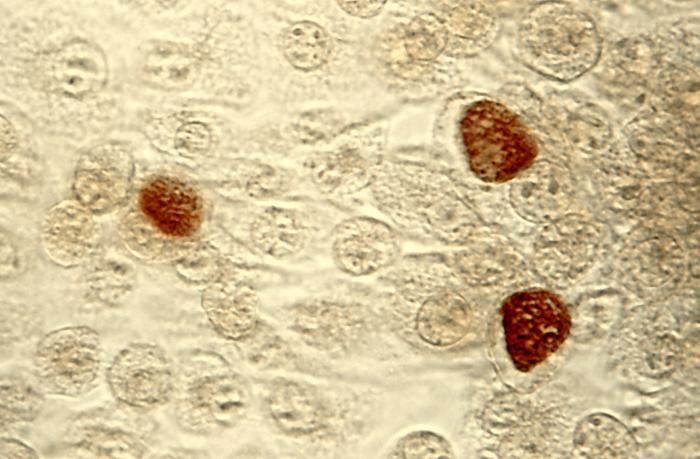
Chlamydia trachomatis (/kləˌmɪdiə/ /trəˈkoʊmətᵻs/), commonly known as chlamydia, is one of four bacterial species in the genus Chlamydia. Chlamydia is a genus of pathogenic bacteria that are obligate intracellular parasites. C. trachomatis is a Gram-negative bacterium. It is ovoid in shape and nonmotile. The bacteria are nonspore-forming, but the elementary bodies act like spores when released into the host. The inclusion bodies of C. trachomatis were first described in 1907 by Stanislaus von Prowazek and Ludwig Halberstädter during research on trachoma. C. trachomatis agent was first cultured in the yolk sacs of eggs by Professor Tang Fei-fan, et al. in 1957.
Contents
- Time lapse video of the chlamydia trachomatis developmental cycle
- Life cycle of chlamydia trachomatis
- Identification
- Clinical significance
- Presentation
- Prevalence
- Treatment
- Laboratory tests
- References
Disorders caused by C. trachomatis include chlamydia, trachoma, lymphogranuloma venereum, nongonococcal urethritis, cervicitis, salpingitis, pelvic inflammatory disease, and pneumonia.
C. trachomatis includes three human biovars:
Many C. trachomatis strains have an extrachromosomal plasmid.
Chlamydia species can exchange DNA between the different strains, thus the evolution of new strains is common.
Life cycle of chlamydia trachomatis
Identification
Chlamydia species are readily identified and distinguished from other Chlamydia species using DNA-based tests.
Most strains of C. trachomatis are recognized by monoclonal antibodies (mAbs) to epitopes in the VS4 region of MOMP. However, these mAbs may also cross-react with two other Chlamydia species, C. suis and C. muridarum.
Clinical significance
Clinical signs and symptoms of C. trachomatis infection and gonorrhea infection are indistinguishable. Both are common causes of urethritis. C. trachomatis is the single most important infectious agent associated with blindness (trachoma); about 84 million worldwide suffer C. trachomatis eye infections and 8 million are blinded as a result of the infection.
Presentation
Most people infected with C. trachomatis are asymptomatic. However, the bacteria can present in one of three ways: genitourinary, pulmonary, and ocular. Genitourinary cases can include genital discharge, vaginal bleeding or pruritus, and dysuria.
Prevalence
Three times as many women as men are diagnosed with genitourinary C. trachomatis infections. Women aged 15–19 have the highest prevalence, followed by women aged 20–24, although the rate of increase of diagnosis is greater for men than for women. Risk factors for genitourinary infections include unprotected sex with multiple partners, lack of condom use, and living in an urban area.
Pulmonary infections can occur in infants born to women with active chlamydia infections, although the rate of infection is less than 10%.
Ocular infections take the form of conjunctivitis or trachoma, both in adults and children. Trachoma is the primary source of infectious blindness in some parts of rural Africa and Asia and is a neglected tropical disease that has been targeted by the World Health Organization for elimination by 2020.
Treatment
Treatment depends on the infection site, age of the patient, and whether another infection is present. Having a C. trachomatis and one or more other sexually transmitted infections at the same time is possible. Treatment is often done with both partners simultaneously to prevent reinfection. C. trachomatis may be treated with several antibiotic medications, including azithromycin, erythromycin, or ofloxacin.
Azythromycin and doxycycline have equal efficacy to treat C. trachomatis with 97 and 98 percent success respectively. Treatment with doxycycline generic 2x1 100mg for 7 days has equal success with expensive delayed-released doxycycline 1x 200mg for 7 days.
If treatment is necessary during pregnancy, levofloxacin, ofloxacin, and doxycycline are not prescribed. In the case of a patient who is pregnant, the medications typically prescribed are azithromycin, amoxicillin, and erythromycin. Amoxicillin has fewer side effects than the other medications for treating antenatal C. trachomatis infection. Retesting during pregnancy can be performed three weeks after treatment. If the risk of reinfection is high, screening can be repeated throughout pregnancy.
If the infection has progressed, ascending the reproductive tract and pelvic inflammatory disease develops, damage to the fallopian tubes may have already occurred. In most cases, the C. trachomatis infection is then treated on an outpatient basis with azithromycin or doxycycline. Treating the mother of an infant with C. trachomatis of the eye, which can evolve into a pneumonia, is recommended.