
ICD-9-CM 331.82 DiseasesDB 3800 | ICD-10 G31.8 OMIM 127750 | |
 | ||
Dementia with Lewy bodies (DLB) is a type of dementia that worsens over time. Additional symptoms may include fluctuations in alertness, visual hallucinations, slowness of movement, trouble walking, and rigidity. Excessive movement during sleep and mood changes such as depression are also common.
Contents
- Signs and symptoms
- Cause
- Pathophysiology
- Diagnosis
- Management
- Medications
- Caregiving
- Epidemiology
- History
- Notable cases
- References
The cause is unknown. Typically, no family history of the disease exists among those affected. The underlying mechanism involves the buildup of Lewy bodies, clumps of alpha-synuclein protein in neurons. It is classified as a neurodegenerative disorder. A diagnosis may be suspected based on symptoms, with blood tests and medical imaging done to rule out other possible causes. The differential diagnosis includes Parkinson's and Alzheimer's.
No cure for DLB is known. Treatments try to improve mental, psychiatric, and motor symptoms. Acetylcholinesterase inhibitors, such as donepezil, may provide some benefit. Some motor problems may improve with levodopa. Antipsychotics, even for hallucinations, should generally be avoided due to side effects.
DLB is the most common cause of dementia after Alzheimer's and vascular dementia. It typically begins after the age of 50. About 0.1% of those over 65 are affected. Males appear to be more commonly affected than females. In the late part of the disease, people may depend entirely on others for their care. Life expectancy following diagnosis is about eight years. The abnormal deposits that cause the disease were discovered in 1912 by Frederic Lewy.
Signs and symptoms
The presenting symptom of dementia with Lewy bodies is often cognitive dysfunction, though dementia eventually occurs in all individuals with DLB. In contrast to Alzheimer's disease (AD), in which memory loss is the first symptom, those with DLB first experience impaired attention, executive function, and visuospatial function, while memory is affected later. These impairments present as driving difficulty, such as becoming lost, misjudging distances, or as impaired job performance. In terms of cognitive testing, individuals may have problems with figure copying as a result of visuospatial impairment, with clock-drawing due to executive function impairment, and difficulty with serial sevens as a result of impaired attention. Short-term memory and orientation to time and place remain intact in the earlier stages of the disease.
While the specific symptoms in a person with DLB may vary, core features include: fluctuating cognition with great variations in attention and alertness from day to day and hour to hour, recurrent visual hallucinations (observed in 75% of people with DLB), and motor features of Parkinson's disease. Suggestive symptoms are rapid eye movement (REM)-sleep behavior disorder and abnormalities detected in PET or SPECT scans. REM sleep behavior disorder (RBD) often is a symptom first recognized by the patient's caretaker. RBD includes vivid dreaming, with persistent dreams, purposeful or violent movements, and falling out of bed. Benzodiazepines, anticholinergics, surgical anesthetics, some antidepressants, and over-the-counter drug cold remedies may cause acute confusion, delusions, and hallucinations.
Tremors are less common in DLB than in Parkinson's disease. Parkinsonian features may include shuffling gait, reduced arm-swing during walking, blank expression (reduced range of facial expression), stiffness of movements, ratchet-like cogwheeling movements, low speech volume, sialorrhea, and difficulty swallowing. Also, DLB patients often experience problems with orthostatic hypotension, including repeated falls, fainting, and transient loss of consciousness. Sleep-disordered breathing, a problem in multiple system atrophy, also may be a problem.
One of the most critical and distinctive clinical features of the disease is hypersensitivity to neuroleptic and antiemetic medications that affect dopaminergic and cholinergic systems. In the worst cases, a patient treated with these medications could become catatonic, lose cognitive function, or develop life-threatening muscle rigidity. Some commonly used medications that should be used with great caution, if at all, for people with DLB, are chlorpromazine, haloperidol, or thioridazine.
Visual hallucinations in people with DLB most commonly involve perception of people or animals that are not there, and may reflect Lewy bodies or AD pathology in the temporal lobe. Delusions may include reduplicative paramnesia and other elaborate misperceptions or misinterpretations. These hallucinations are not necessarily disturbing, and in some cases, the person with DLB may have insight into the hallucinations and even be amused by them, or be conscious they are not real. People with DLB also may have problems with vision, including double vision, and misinterpretation of what they see, for example, mistaking a pile of socks for snakes or a clothes closet for the bathroom.
Cause
The major cause of DLB is not well understood yet, but a genetic link with the PARK11 gene has been described. As with Alzheimer's disease and Parkinson's disease, most cases of DLB appear sporadically and DLB is not thought to have a strong hereditary link. As with Alzheimer's disease, the LBD risk is heightened with inheritance of the ε4 allele of the apolipoprotein E (APOE).
In DLB, loss of cholinergic (acetylcholine-producing) neurons is thought to account for degeneration of cognitive function (similar to Alzheimer's), while the death of dopaminergic (dopamine-producing) neurons appears to be responsible for degeneration of motor control (similar to Parkinson's) – in some ways, therefore, LBD resembles both disorders.
Pathophysiology
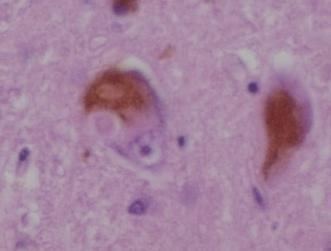
Pathologically, DLB is characterized by the development of abnormal collections of (alpha-synuclein) protein within the cytoplasm of neurons (known as Lewy bodies). These intracellular collections of protein have similar structural features to "classical" Lewy bodies, seen subcortically in Parkinson's disease. Additionally, those affected by DLB experience a loss of dopamine-producing neurons (in the substantia nigra) in a manner similar to that seen in Parkinson's disease. A loss of acetylcholine-producing neurons (in the basal nucleus of Meynert and elsewhere) similar to that seen in Alzheimer's disease also is known to occur in those with DLB. Cerebral atrophy also occurs as the cerebral cortex degenerates. Autopsy series have revealed the pathology of DLB is often concomitant with the pathology of Alzheimer's disease. That is, when Lewy body inclusions are found in the cortex, they often co-occur with Alzheimer's disease pathology found primarily in the hippocampus, including senile plaques (deposited beta-amyloid protein), and granulovacuolar degeneration (grainy deposits within and a clear zone around hippocampal neurons). Neurofibrillary tangles (abnormally phosphorylated tau protein) are less common in DLB, although they are known to occur, and astrocyte abnormalities are also known to occur. Presently, whether DLB is an Alzheimer's variant or a separate disease entity is not clear. Unlike Alzheimer's disease, the brain may appear grossly normal with no visible signs of atrophy.
Diagnosis
The symptoms of DLB overlap clinically with those of Alzheimer's disease and Parkinson's disease, but are associated more commonly with the latter. Because of this overlap, early DLB is often misdiagnosed. The overlap of neuropathological and presenting symptoms (cognitive, emotional, and motor) may make an accurate differential diagnosis difficult. In fact, DLB often is confused in its early stages with Alzheimer's disease and/or vascular dementia (multi-infarct dementia). However, while Alzheimer’s disease usually begins gradually, DLB frequently has a rapid or acute onset, with an especially rapid cognitive and physical decline in the first few months. Thus, DLB tends to progress more rapidly than Alzheimer’s disease. Despite the difficulty, a prompt diagnosis is important because of the risks of sensitivity to certain neuroleptic (antipsychotic) medications and because appropriate treatment of symptoms may improve life for both the person with DLB and the person's caregivers.
Dementia with Lewy bodies is distinguished from the dementia that sometimes occurs in Parkinson's disease by the time frame in which dementia symptoms appear relative to Parkinson symptoms. Parkinson's disease with dementia (PDD) would be the diagnosis when the onset of dementia is more than a year after the onset of Parkinsonian symptoms. DLB is diagnosed when cognitive symptoms begin at the same time or within a year of Parkinson symptoms.
Management
No cure for dementia with Lewy bodies is known. Treatment may offer symptomatic benefit, but remains palliative in nature. Current treatment modalities are divided into pharmaceutical and caregiving.
Medications
Pharmaceutical management, as with Parkinson's disease, involves striking a balance between treating the motor, emotive, and cognitive symptoms. Motor symptoms appear to respond somewhat to the medications used to treat Parkinson's disease (e.g. levodopa), while cognitive issues may improve with medications for Alzheimer's disease such as donepezil. Medications used in the treatment of ADHD (e.g. methylphenidate) might improve cognition or daytime sleepiness; however, medications for both Parkinson's disease and ADHD increase levels of the chemical dopamine in the brain, so increase the risk of hallucinations with those classes of pharmaceuticals.
Treatment of the movement and cognitive portions of the disease may worsen hallucinations and psychosis, while treatment of hallucinations and psychosis with antipsychotics may worsen parkinsonian or ADHD symptoms in DLB, such as tremor or rigidity and lack of concentration or impulse control. Physicians may find the use of cholinesterase inhibitors represents the treatment of choice for cognitive problems and donepezil (Aricept), rivastigmine (Exelon), and galantamine (Reminyl) may be recommended as a means to help with these problems and to slow or prevent the decline of cognitive function. DLB may be more responsive to donepezil than Alzheimer's disease. Memantine also may be useful. Levocarb may help with movement problems, but in some cases, as with dopamine agonists, may tend to aggravate psychosis in people with DLB. Clonazepam may help with rapid eye movement behavior disorder; table salt or antihypotensive medications may help with fainting and other problems associated with orthostatic hypotension. Botulinum toxin injections in the parotid glands may help with sialorrhea. Other medications, especially stimulants such as the ADHD drug methylphenidate (Ritalin) and modafinil, may improve daytime alertness, but as with the antiparkinsonian drug Levocarb, antihyperkinetics such as Ritalin increase the risk of psychosis. Experts advise extreme caution in the use of antipsychotic medication in people with DLB because of their sensitivity to these agents. When these medications must be used, atypical antipsychotics are preferred to typical antipsychotics; a very low dose should be tried initially and increased slowly, and patients should be carefully monitored for adverse reactions to the medications.
Due to hypersensitivity to neuroleptics, preventing DLB patients from taking these medications is important. People with DLB are at risk for neuroleptic malignant syndrome, a life-threatening illness, because of their sensitivity to these medications, especially the older typical antipsychotics, such as haloperidol. Other medications, including medications for urinary incontinence and the antihistamine medication diphenhydramine (Benadryl), also may worsen confusion.
Caregiving
Because DLB gradually renders people incapable of tending to their own needs, caregiving is very important and must be managed carefully over the course of the disease. Caring for people with DLB involves adapting the home environment, schedule, activities, and communications to accommodate declining cognitive skills and parkinsonian symptoms.
People with DLB may swing dramatically between good days, with high alertness and few cognitive or movement problems, and bad days, and the level of care they require thus may vary widely and unpredictably. Sharp changes in behavior may be due to the day-to-day variability of DLB, but they also may be triggered by changes in the schedule or home environment, or by physical problems, such as constipation, dehydration, bladder infection, injuries from falls, and other problems they may not be able to convey to caregivers. Potential physical problems always should be taken into consideration when an individual with DLB becomes agitated.
As hallucinations and delusions are not dangerous or troubling to the person with DLB, caregivers not disabusing patients of them may be best. Often, the best approach is benign neglect—acknowledging, but not encouraging or agreeing. Trying to talk the DLB patient out of his delusion may be frustrating to caregivers and discouraging to patients, sometimes provoking anger or dejection. When misperceptions, hallucinations, and the behaviors stemming from these become troublesome, caregivers should try to identify and eliminate environmental triggers, and perhaps, offer cues or "therapeutic white lies" to steer patients out of trouble. Physicians may prescribe low doses of atypical antipsychotics, such as quetiapine, for psychosis and agitation in DLB. A small clinical trial found that about half of DLB patients treated with low doses of quetiapine experienced a significant reduction in these symptoms. Unfortunately, several participants in the study had to discontinue treatment because of side effects, such as excessive daytime sleepiness or orthostatic hypotension.
Changes in the schedule or environment, delusions, hallucinations, misperceptions, and sleep problems also may trigger behavior changes. It can help people with DLB to encourage exercise, simplify the visual environment, stick to a routine, and avoid asking too much (or too little) of them. Speaking slowly and sticking to essential information improves communication. The potential for visual misperception and hallucinations, in addition to the risk of abrupt and dramatic swings in cognition and motor impairment, should put families on alert to the dangers of driving with DLB.
Epidemiology
Currently, an estimated 60 to 75% of diagnosed dementias are of the Alzheimer's and mixed (Alzheimer's and vascular dementia) type, 10 to 15%are Lewy body type, with the remaining types being of an entire spectrum of dementias, including frontotemporal lobar degeneration (Pick's disease), alcoholic dementia, pure vascular dementia, etc. Dementia with Lewy bodies tends to be under-recognized. Dementia with Lewy bodies is slightly more prevalent in men than women. DLB increases in prevalence with age; the mean age at presentation is 75 years.
Dementia with Lewy bodies affects about one million individuals in the United States.
History
Frederic Lewy (1885–1950) was first to discover the abnormal protein deposits ("Lewy body inclusions") in the early 1900s. Dementia with Lewy bodies was first described by Japanese psychiatrist and neuropathologist Kenji Kosaka in 1976. DLB started to be diagnosed in the mid-1990s after the discovery of alpha-synuclein staining first highlighted Lewy bodies in the cortex of post mortem brains of a subset of dementia patients. DLB was briefly mentioned in the DSM-IV-TR (published in 2000) under "Dementia Due to Other General Medical Conditions." It is listed in DSM-5 as "Major or Mild Neurocognitive Disorder with Lewy Bodies."