
ICD-9-CM 788.3 MedlinePlus 003142 | ICD-10 N39.3-N39.4, R32 DiseasesDB 6764 eMedicine med/2781 | |
 | ||
Similar Artificial urinary sphincter, Pelvic organ prolapse, Stress incontinence | ||
Urinary incontinence (UI), also known as involuntary urination, is any leakage of urine. It is a common and distressing problem, which may have a large impact on quality of life. It is twice as common in women as in men. pregnancy, childbirth, and menopause are major risk factors. It has been identified as an important issue in geriatric health care. Urinary incontinence is often a result of an underlying medical condition but is under-reported to medical practitioners. enuresis is often used to refer to urinary incontinence primarily in children, such as nocturnal enuresis (bed wetting).
Contents
- Causes
- Mechanism
- Children
- Diagnosis
- Types
- Treatment
- Exercises
- Devices
- Medications
- Surgery
- Epidemiology
- Women
- Men
- History
- References
There are four main types of incontinence:
Treatments include pelvic floor muscle training, bladder training, and electrical stimulation. The benefit of medications is small and long term safety is unclear.
Causes
The most common types of urinary incontinence in women are stress urinary incontinence and urge urinary incontinence. Women with both problems have mixed urinary incontinence. After menopause, estrogen production decreases and in some women urethral tissue will demonstrate atrophy with the tissue of the urethra becoming weaker and thinner. Stress urinary incontinence is caused by loss of support of the urethra which is usually a consequence of damage to pelvic support structures as a result of childbirth. It is characterized by leaking of small amounts of urine with activities which increase abdominal pressure such as coughing, sneezing and lifting. Additionally, frequent exercise in high-impact activities can cause athletic incontinence to develop. Urge urinary incontinence is caused by uninhibited contractions of the detrusor muscle . It is characterized by leaking of large amounts of urine in association with insufficient warning to get to the bathroom in time.
Mechanism
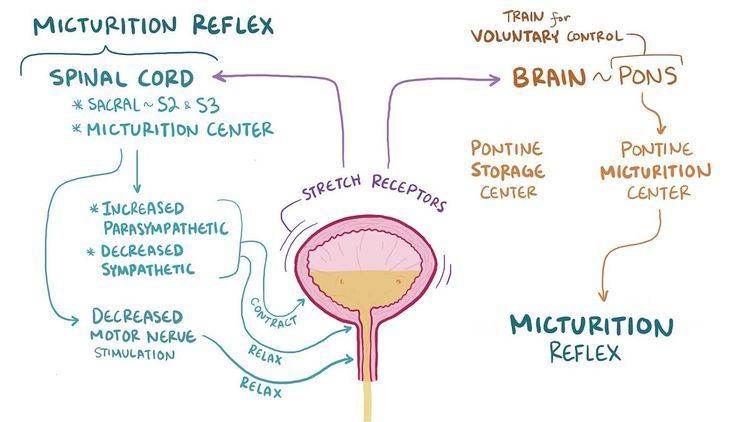
Continence and micturition involve a balance between urethral closure and detrusor muscle activity. Urethral pressure normally exceeds bladder pressure, resulting in urine remaining in the bladder. The proximal urethra and bladder are both within the pelvis. Intra abdominal pressure increases (from coughing and sneezing) are transmitted to both urethra and bladder equally, leaving the pressure differential unchanged, resulting in continence. Normal voiding is the result of changes in both of these pressure factors: urethral pressure falls and bladder pressure rises.
The body stores urine — water and wastes removed by the kidneys — in the urinary bladder, a balloon-like organ. The bladder connects to the urethra, the tube through which urine leaves the body.
During urination, detrusor muscles in the wall of the bladder contract, forcing urine out of the bladder and into the urethra. At the same time, sphincter muscles surrounding the urethra relax, letting urine pass out of the body. Incontinence will occur if the bladder muscles suddenly contract (detrusor muscle) or muscles surrounding the urethra suddenly relax (sphincter muscles).
Children
Urination, or voiding, is a complex activity. The bladder is a balloonlike muscle that lies in the lowest part of the abdomen. The bladder stores urine, then releases it through the urethra, the canal that carries urine to the outside of the body. Controlling this activity involves nerves, muscles, the spinal cord and the brain.
The bladder is made of two types of muscles: the detrusor, a muscular sac that stores urine and squeezes to empty, and the sphincter, a circular group of muscles at the bottom or neck of the bladder that automatically stay contracted to hold the urine in and automatically relax when the detrusor contracts to let the urine into the urethra. A third group of muscles below the bladder (pelvic floor muscles) can contract to keep urine back.
A baby's bladder fills to a set point, then automatically contracts and empties. As the child gets older, the nervous system develops. The child's brain begins to get messages from the filling bladder and begins to send messages to the bladder to keep it from automatically emptying until the child decides it is the time and place to void.
Failures in this control mechanism result in incontinence. Reasons for this failure range from the simple to the complex.
Diagnosis
Patients with incontinence should be referred to a medical practitioner specializing in this field. Urologists specialize in the urinary tract, and some urologists further specialize in the female urinary tract. A urogynecologist is a gynecologist who has special training in urological problems in women. Family physicians and internists see patients for all kinds of complaints, and are well trained to diagnose and treat this common problem. These primary care specialists can refer patients to urology specialists if needed.
A careful history taking is essential especially in the pattern of voiding and urine leakage as it suggests the type of incontinence faced. Other important points include straining and discomfort, use of drugs, recent surgery, and illness.
The physical examination will focus on looking for signs of medical conditions causing incontinence, such as tumors that block the urinary tract, stool impaction, and poor reflexes or sensations, which may be evidence of a nerve-related cause.
A test often performed is the measurement of bladder capacity and residual urine for evidence of poorly functioning bladder muscles.
Other tests include:
Patients are often asked to keep a diary for a day or more, up to a week, to record the pattern of voiding, noting times and the amounts of urine produced.
Research projects that assess the efficacy of anti-incontinence therapies often quantify the extent of urinary incontinence. The methods include the 1-h pad test, measuring leakage volume; using a voiding diary, counting the number of incontinence episodes (leakage episodes) per day; and assessing of the strength of pelvic floor muscles, measuring the maximum vaginal squeeze pressure.
Types
Treatment
Treatment options range from conservative treatment, behavior management, bladder retraining, pelvic floor therapy, collecting devices (for men), fixer-occluder devices for incontinence (in men), medications and surgery. The success of treatment depends on the correct diagnoses. Weight loss is recommended in those who are obese.
Exercises
Exercising the muscles of the pelvis such as with Kegel exercises are a first line treatment for women with stress incontinence. Efforts to increase the time between urination, known as bladder training, is recommended in those with urge incontinence. Both these may be used in those with mixed incontinence.
Small vaginal cones of increasing weight may be used to help with exercise. They seem to be better than no active treatment in women with stress urinary incontinence, and have similar effects to training of pelvic floor muscles or electrostimulation.
biofeedback uses measuring devices to help the patient become aware of his or her body's functioning. By using electronic devices or diaries to track when the bladder and urethral muscles contract, the patient can gain control over these muscles. Biofeedback can be used with pelvic muscle exercises and electrical stimulation to relieve stress and urge incontinence.
Time voiding while urinating and bladder training are techniques that use biofeedback. In time voiding, the patient fills in a chart of voiding and leaking. From the patterns that appear in the chart, the patient can plan to empty his or her bladder before he or she would otherwise leak. Biofeedback and muscle conditioning, known as bladder training, can alter the bladder's schedule for storing and emptying urine. These techniques are effective for urge and overflow incontinence
A 2013 randomized controlled trial found no benefit of adding biofeedback to pelvic floor muscle exercise in stress urinary incontinence, but observing improvements in both groups. In another randomized controlled trial the addition of biofeedback to the training of pelvic floor muscles for the treatment of stress urinary incontinence, improved pelvic floor muscle function, reduced urinary symptoms, and improved of the quality of life.
Preoperative pelvic floor muscle training (PFMT) in men undergoing radical prostatectomy was not effective in reducing urinary incontinence.
Alternative exercises have been studied for stress urinary incontinence in women. Evidence was insufficient to support the use of Paula method, abdominal muscle training, Pilates, Tai Chi, breathing exercises, postural training, and generalized fitness.
Devices
Individuals who continue to experience urinary incontinence need to find a management solution that matches their individual situation. The use of devices has not been well studied in women as of 2014.
Medications
A number of medications exist to treat incontinence including: fesoterodine, tolterodine and oxybutynin. While a number appear to have a small benefit, the risk of side effects are a concern. For every ten or so people treated only one will become able to control their urine and all medication are of similar benefit.
Medications are not recommended for those with stress incontinence and are only recommended in those who have urge incontinence who do not improve with bladder training.
Surgery
Surgery may be used to help stress or overflow incontinence. Common surgical techniques for stress incontinence include slings, tension-free vaginal tape, and bladder suspension among others. Urodynamic testing seems to confirm that surgical restoration of vault prolapse can cure motor urge incontinence. In those with problems following prostate surgery there is little evidence regarding the use of surgery.
Epidemiology
Globally, up to 35% of the population over the age of 60 years is estimated to be incontinent. In 2014, urinary leakage affected between 30% and 40% of people over 65 years of age living in their own homes or apartments in the U.S. Twenty-four percent of older adults in the U.S. have moderate or severe urinary incontinence that should be treated medically.
Bladder control problems have been found to be associated with higher incidence of many other health problems such as obesity and diabetes. Difficulty with bladder control results in higher rates of depression and limited activity levels.
Incontinence is expensive both to individuals in the form of bladder control products and to the health care system and nursing home industry. Injury related to incontinence is a leading cause of admission to assisted living and nursing care facilities. More than 50% of nursing facility admissions are related to incontinence.
Children
Incontinence happens less often after age 5: About 10 percent of 5-year-olds, 5 percent of 10-year-olds, and 1 percent of 18-year-olds experience episodes of incontinence. It is twice as common in girls as in boys.
Women
Bladder symptoms affect women of all ages. However, bladder problems are most prevalent among older women. Women over the age of 60 years are twice as likely as men to experience incontinence; one in three women over the age of 60 years are estimated to have bladder control problems. One reason why women are more affected is the weakening of pelvic floor muscles by pregnancy.
Men
Men tend to experience incontinence less often than women, and the structure of the male urinary tract accounts for this difference. It is common with prostate cancer treatments. Both women and men can become incontinent from neurologic injury, congenital defects, strokes, multiple sclerosis, and physical problems associated with aging.
While urinary incontinence affects older men more often than younger men, the onset of incontinence can happen at any age. Estimates in the mid-2000s suggested that 17 percent of men over age 60, an estimated 600,000 men, experienced urinary incontinence, with this percentage increasing with age.
History
The management of urinary incontinence with pads is mentioned in the earliest medical book known, the Ebers Papyrus (1500 BC).