
Symbol APP InterPro IPR013803 SUPERFAMILY 2lfm HUGO 620 | Pfam PF03494 SCOP 2lfm TCDB 1.C.50 OMIM 104760 | |
 | ||
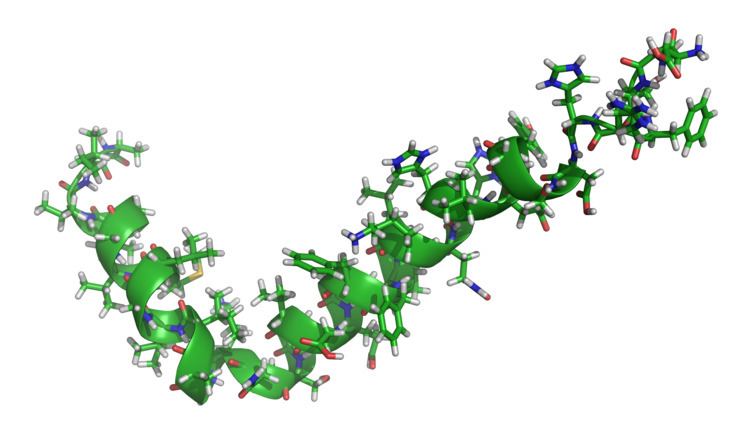
Amyloid beta 42 peptide ab42 2
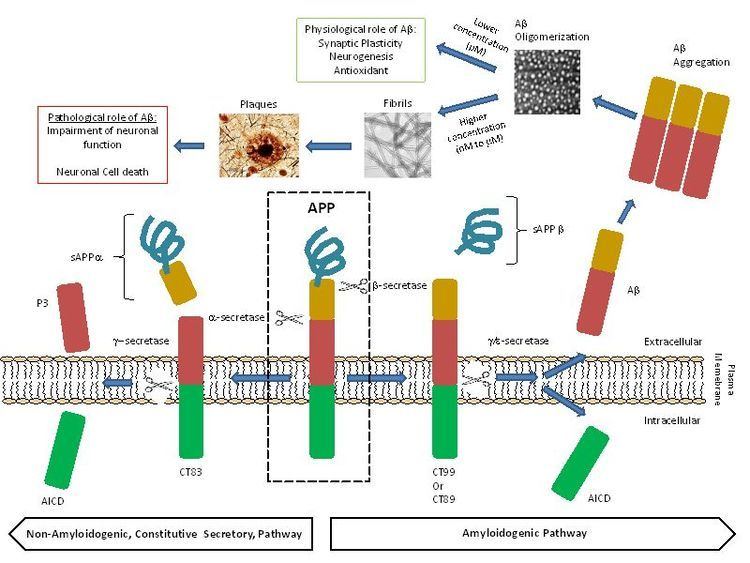
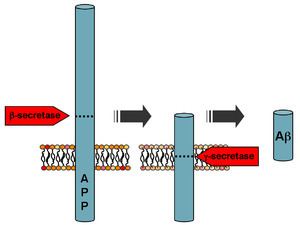
Amyloid beta (Aβ or Abeta) denotes peptides of 36–43 amino acids that are crucially involved in Alzheimer's disease as the main component of the amyloid plaques found in the brains of Alzheimer patients. The peptides result from the amyloid precursor protein (APP), which is cleaved by beta secretase and gamma secretase to yield Aβ. Aβ molecules can aggregate to form flexible soluble oligomers which may exist in several forms. It is now believed that certain misfolded oligomers (known as "seeds") can induce other Aβ molecules to also take the misfolded oligomeric form, leading to a chain reaction akin to a prion infection. The seeds or the resulting amyloid plaques are toxic to nerve cells. The other protein implicated in Alzheimer's disease, tau protein, also forms such prion-like misfolded oligomers, and there is some evidence that misfolded Aβ can induce tau to misfold.
Contents
- Amyloid beta 42 peptide ab42 2
- Amyloid beta protein dynamics
- Normal function
- Disease associations
- Alzheimers disease
- Formation
- Genetics
- Structure and toxicity
- Intervention strategies
- Circadian rhythm of amyloid beta
- Measuring amyloid beta
- Post mortum or in tissue biopsies
- References
A recent study suggested that APP and its amyloid potential is of ancient origins, dating as far back as early deuterostomes.
Amyloid beta protein dynamics
Normal function
The normal function of Aβ is not well understood. Though some animal studies have shown that the absence of Aβ does not lead to any loss of physiological function, several potential activities have been discovered for Aβ, including activation of kinase enzymes, protection against oxidative stress, regulation of cholesterol transport, functioning as a transcription factor, and anti-microbial activity (potentially associated with Aβ's pro-inflammatory activity).
The glymphatic system clears metabolic waste from the mammalian brain, and in particular beta amyloids. The rate of removal is significantly increased during sleep. However, the significance of the glymphatic system is unknown in clearance of Aβ.
Disease associations
Aβ is the main component of amyloid plaques (extracellular deposits found in the brains of patients with Alzheimer's disease). Similar plaques appear in some variants of Lewy body dementia and in inclusion body myositis (a muscle disease), while Aβ can also form the aggregates that coat cerebral blood vessels in cerebral amyloid angiopathy. The plaques are composed of a tangle of regularly ordered fibrillar aggregates called amyloid fibers, a protein fold shared by other peptides such as the prions associated with protein misfolding diseases.
Alzheimer's disease
Recent research suggests that soluble oligomeric forms of the peptide may be causative agents in the development of Alzheimer's disease. It is generally believed that Aβ oligomers are the most toxic. The ion channel hypothesis postulates that oligomers of soluble, non-fibrillar Aβ form membrane ion channels allowing the unregulated calcium influx into neurons that underlies disrupted calcium ion homeostasis and apoptosis seen in Alzheimer's disease. A number of genetic, cell biology, biochemical and animal studies support the concept that Aβ plays a central role in the development of Alzheimer’s disease pathology.
Brain Aβ is elevated in patients with sporadic Alzheimer’s disease. Aβ is the main constituent of brain parenchymal and vascular amyloid; it contributes to cerebrovascular lesions and is neurotoxic. It is unresolved how Aβ accumulates in the central nervous system and subsequently initiates the disease of cells. Some researchers have found that the Aβ oligomers induce some of the symptoms of Alzheimer's Disease by competing with insulin for binding sites on the insulin receptor, thus impairing glucose metabolism in the brain. Significant efforts have been focused on the mechanisms responsible for Aβ production, including the proteolytic enzymes gamma- and β-secretases which generate Aβ from its precursor protein, APP (amyloid precursor protein). Aβ circulates in plasma, cerebrospinal fluid (CSF) and brain interstitial fluid (ISF) mainly as soluble Aβ40 Senile plaques contain both Aβ40 and Aβ42, while vascular amyloid is predominantly the shorter Aβ40. Several sequences of Aβ were found in both lesions. Generation of Aβ in the CNS may take place in the neuronal axonal membranes after APP-mediated axonal transport of β-secretase and presenilin-1.
Increases in either total Aβ levels or the relative concentration of both Aβ40 and Aβ42 (where the former is more concentrated in cerebrovascular plaques and the latter in neuritic plaques) have been implicated in the pathogenesis of both familial and sporadic Alzheimer's disease. Due to its more hydrophobic nature, the Aβ42 is the most amyloidogenic form of the peptide. However the central sequence KLVFFAE is known to form amyloid on its own, and probably forms the core of the fibril.
The "amyloid hypothesis", that the plaques are responsible for the pathology of Alzheimer's disease, is accepted by the majority of researchers but is by no means conclusively established. An alternative hypothesis is that amyloid oligomers rather than plaques are responsible for the disease. Mice that are genetically engineered to express oligomers but not plaques (APPE693Q) develop the disease. Furthermore, mice that are in addition engineered to convert oligomers into plaques (APPE693Q X PS1ΔE9), are no more impaired than the oligomer only mice. Intra-cellular deposits of tau protein are also seen in the disease, and may also be implicated, as has aggregation of alpha synuclein.
Currently, research is being done using biomarkers and ELISA tests to determine levels of amyloid beta so blood tests can detect Alzheimer's Disease in its early stages. Of 24 biomarkers, 3 were confirmed to be reliable identification markers of AD patients.
Formation
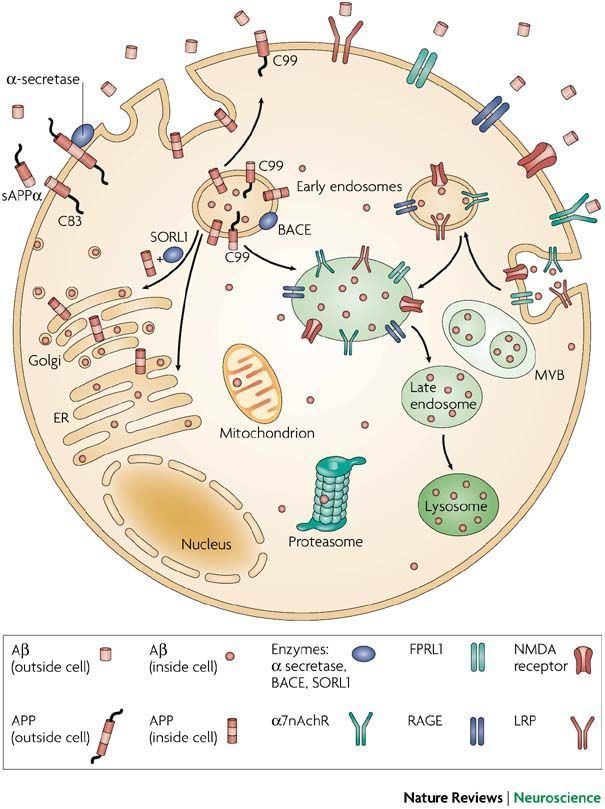
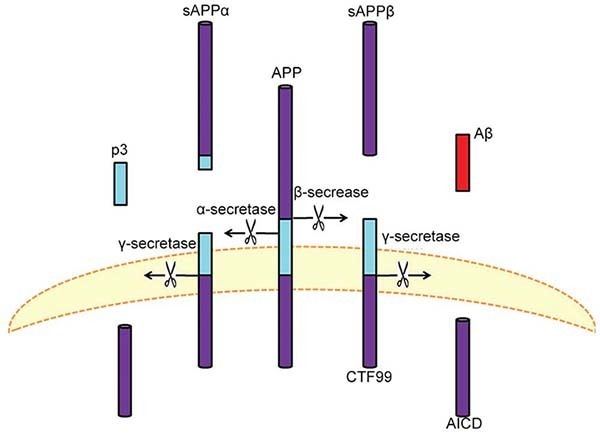
Aβ is formed after sequential cleavage of the amyloid precursor protein (APP), a transmembrane glycoprotein of undetermined function. APP can be cleaved by the proteolytic enzymes α-, β- and γ-secretase; Aβ protein is generated by successive action of the β and γ secretases. The γ secretase, which produces the C-terminal end of the Aβ peptide, cleaves within the transmembrane region of APP and can generate a number of isoforms of 30-51 amino acid residues in length. The most common isoforms are Aβ40 and Aβ42; the longer form is typically produced by cleavage that occurs in the endoplasmic reticulum, while the shorter form is produced by cleavage in the trans-Golgi network. The Aβ40 form is the more common of the two, but Aβ42 is the more fibrillogenic and is thus associated with disease states. Mutations in APP associated with early-onset Alzheimer's have been noted to increase the relative production of Aβ42, and thus one suggested avenue of Alzheimer's therapy involves modulating the activity of β and γ secretases to produce mainly Aβ40. Aβ is destroyed by several amyloid-degrading enzymes including neprilysin.
Genetics
Autosomal-dominant mutations in APP cause hereditary early-onset Alzheimer's disease (a.k.s. familial AD). This form of AD accounts for no more than 10% of all cases, and the vast majority of AD is not accompanied by such mutations. However, familial Alzheimer disease is likely to result from altered proteolytic processing.
The gene for amyloid precursor protein is located on chromosome 21, and accordingly people with Down syndrome have a very high incidence of Alzheimer's disease.
Structure and toxicity
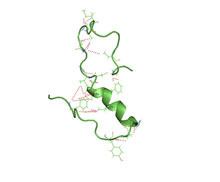
Amyloid beta is commonly thought to be intrinsically unstructured, meaning that in solution it does not acquire a unique tertiary fold but rather populates a set of structures. As such, it cannot be crystallized and most structural knowledge on amyloid beta comes from NMR and molecular dynamics. Early NMR-derived models of a 26-aminoacid polypeptide from amyloid beta (Aβ 10-35) show a collapsed coil structure devoid of significant secondary structure content. However, the most recent (2012) NMR structure of (Aβ 1-40) has significant secondary and tertiary structure. Replica exchange molecular dynamics studies suggested that amyloid beta can indeed populate multiple discrete structural states; more recent studies identified a multiplicity of discrete conformational clusters by statistical analysis. By NMR-guided simulations, amyloid beta 1-40 and amyloid beta 1-42 also seem to feature highly different conformational states, with the C-terminus of amyloid beta 1-42 being more structured than that of the 1-40 fragment.
Structural information on the oligomeric state of amyloid beta is still sparse as of 2010. Low-temperature and low-salt conditions allowed to isolate pentameric disc-shaped oligomers devoid of beta structure. In contrast, soluble oligomers prepared in the presence of detergents seem to feature substantial beta sheet content with mixed parallel and antiparallel character, different from fibrils; computational studies suggest an antiparallel beta-turn-beta motif instead for membrane-embedded oligomers.
The mechanism by which amyloid beta may damage and kill neurons is by generating reactive oxygen species during the process of its self-aggregation. When this occurs on the membrane of neurons it causes lipid peroxidation and the generation of a toxic aldehyde called 4-hydroxynonenal which, in turn, impairs the function of ion-motive ATPases, glucose transporters and glutamate transporters. As a result, amyloid beta promotes depolarization of the synaptic membrane, excessive calcium influx and mitochondrial impairment.
Intervention strategies
Researchers in Alzheimer's disease have identified five strategies as possible interventions against amyloid:
β- and γ-secretase are responsible for the generation of Aβ from the release of the intracellular domain of APP, meaning that compounds that can partially inhibit the activity of either β- and γ-secretase are highly sought after. In order to initiate partial inhibition of β- and γ-secretase, a compound is needed that can block the large active site of aspartyl proteases while still being capable of bypassing the blood-brain barrier. To date, human testing has been avoided due to concern that it might interfere with signaling via Notch proteins and other cell surface receptors.
Recent research shows that the wakefulness inducing hormone orexin influences amyloid beta (see below).
The cannabinoid HU-210 has been shown to prevent amyloid beta-promoted inflammation. The endocannabinoids anandamide and noladin ether have also been shown to be neuroprotective against amyloid beta in vitro.
It has been shown that high-cholesterol diets tend to increase Aβ pathology in animals. Modulating cholesterol homeostasis has yielded results that show that chronic use of cholesterol-lowering drugs, such as the statins, is associated with a lower incidence of AD. In APP genetically modified mice, cholesterol-lowering drugs have been shown to reduce overall pathology. While the mechanism is poorly understood it appears that cholesterol-lowering drugs have a direct effect on APP processing.
Chelation therapy, which involves the removal of heavy metals from the body, has also been shown to be beneficial in lowering amyloid plaque levels. This is because Aβ aggregation is somewhat dependent on the metal ions copper and zinc. Zinc in synaptic vesicles, which is under the control of the zinc transporter ZnT3, plays a major role in Aβ formation. The expression of the ZnT3 is significantly lower in Alzheimer’s patients compared to healthy patients. Mice without ZnT3 were found to have much higher plaque formation. Further promoting this concept, Aβ deposition was impeded in APP transgenic mice treated with the antibiotic clioquinol, a known copper/zinc chelator.
Drug therapy has been another approach to treatment. Memantine is an Alzheimer’s drug which has received widespread approval. It is a non-competitive N-methyl-D-aspartate (NMDA) channel blocker. By binding to the NMDA receptor with a higher affinity than Mg2+ ions, memantine is able to inhibit the prolonged influx of Ca2+ ions, particularly from extrasynaptic receptors, which forms the basis of neuronal excitotoxicity. It is an option for the management of patients with moderate to severe Alzheimer's Disease (modest effect). The study showed that 20 mg/day improved cognition, functional ability and behavioural symptoms in patient population.
Another drug under research is liraglutide, which is typically used as a diabetes drug. Treatment with liraglutide yielded cognitive benefits that included improved object and spatial recognition. It enhanced induction and maintenance of long term potentiation (LTP) and paired-pulse facilitation (PPF) in both APP/PS1 and non-genetically altered mice. Other histological benefits include a reduced inflammatory response and an increase in the number of young neurons in the dentate gyrus. The β-amyloid level was also found to be significantly reduced.
Circadian rhythm of amyloid beta
A 2009 report demonstrated that amyloid beta production follows a circadian rhythm, rising when an animal (mouse) or person is awake and falling during sleep. The wakefulness-promoting neuroprotein orexin was shown to be necessary for the circadian rhythm of amyloid beta production. The report suggested that excessive periods of wakefulness (i.e. due to sleep debt) could cause chronic build-up of amyloid beta, which could hypothetically lead to Alzheimer's disease. This is consistent with recent findings that chronic sleep deprivation is associated with early onset Alzheimer's disease.
Melatonin is also involved in circadian rhythm maintenance. Notably, melatonin has been connected with the "sundowning" phenomenon, in which Alzheimer's disease patients that have amyloid plaques in the hypothalamus exhibit exacerbation of Alzheimer's disease symptoms late in the day. This "sundowning" phenomenon could be directly or indirectly related to the recently discovered continuous increase in amyloid beta throughout the day.
Measuring amyloid beta
Imaging compounds, notably Pittsburgh compound B, (6-OH-BTA-1, a thioflavin), can selectively bind to amyloid beta in vitro and in vivo. This technique, combined with PET imaging, has been used to image areas of plaque deposits in Alzheimer's patients.
Post mortum or in tissue biopsies
There are many different ways to measure Amyloid beta. It can be measured semi-quantitatively with immunostaining, which also allows one to determine location. Amyloid beta may be primarily vascular, as in cerebral amyloid angiopathy, or in senile plaques and vascular.
One highly sensitive method is ELISA which is an immunosorbent assay which utilizes a pair of antibodies that recognize Amyloid beta.
Atomic force microscopy, which can visualize nanoscale molecular surfaces, can be used to determine the aggregation state of Amyloid beta in vitro.
Dual polarisation interferometry is an optical technique which can measure the very earliest stages of aggregration and inhibition by measuring the molecular size and densities as the fibrils elongate. These aggregate processes can also be studied on lipid bilayer constructs.