
3DMet B00094 Molar mass 168.1103 g/mol Density 1.87 g/cm³ Appearance White crystals | Formula C5H4N4O3 Melting point 300 °C | |
 | ||
IUPAC ID 7,9-Dihydro-1H-purine-2,6,8(3H)-trione Similar Creatinine, Cholesterol, Triglyceride | ||
Uric acid video organic chemistry
Uric acid is a heterocyclic compound of carbon, nitrogen, oxygen, and hydrogen with the formula C5H4N4O3. It forms ions and salts known as urates and acid urates, such as ammonium acid urate. Uric acid is a product of the metabolic breakdown of purine nucleotides, and it is a normal component of urine. High blood concentrations of uric acid can lead to gout and are associated with other medical conditions including diabetes and the formation of ammonium acid urate kidney stones.
Contents
- Uric acid video organic chemistry
- Chemistry
- Solubility
- Biology
- Genetics
- Medicine
- High uric acid
- Causes of high uric acid
- Gout
- Lesch Nyhan syndrome
- Cardiovascular disease
- Type 2 diabetes
- Metabolic syndrome
- Uric acid stone formation
- Causes of low uric acid
- Multiple sclerosis
- Normalizing low uric acid
- Oxidative stress
- References
Chemistry
Uric acid is a diprotic acid with pKa1 = 5.4 and pKa2 = 10.3. Thus in strong alkali at high pH, it forms the dually-charged full urate ion, but at biological pH or in the presence of bicarbonate ions, it forms the singly-charged hydrogen urate or acid urate ion. As its second ionization is so weak, the full urate salts hydrolyze back to hydrogen urate salts at pH values around neutral. It is aromatic because of conjugated pi bonding in both rings.
As a bicyclic, heterocyclic purine derivative, uric acid does not protonate from an oxygen (−OH) as carboxylic acids do. X-ray diffraction studies on the hydrogen urate ion in crystals of ammonium hydrogen urate, formed in vivo as gouty deposits, reveal that the keto oxygen in the 2 position of the purine structure (on the carbon between two nitrogens in the six-membered ring) exists as an OH group while the two flanking nitrogen atoms at the 1 and 3 positions share the ionic charge in the six-membered pi-resonance-stabilized ring.
Thus, while most organic acids are deprotonated by the ionization of a polar hydrogen–oxygen bond, usually accompanied by some form of resonance stabilization (resulting in a carboxylate ion), uric acid is deprotonated at a nitrogen atom and uses a tautomeric keto/hydroxy group as an electron-withdrawing group to increase the pK1 value. The five-membered ring also possesses a keto group (in the 8 position), flanked by two secondary amino groups (in the 7 and 9 positions), and deprotonation of one of these at high pH could explain the pK2 and behavior as a diprotic acid. Similar tautomeric rearrangement and pi-resonance stabilization would then give the ion some degree of stability.
Calculations seem to indicate that in aqueous solution (and in the gas phase), the singly ionized form has no hydrogens on oxygens and lacks a hydrogen either on nitrogen 9 or on nitrogen 3, whereas the un-ionized uric acid has hydrogens on all four nitrogens. (On the structure shown at the upper-right, the NH at the upper-right on the six-membered ring is "1", counting clockwise around the six-membered ring to "6" for the keto carbon at the top of the six-membered ring. The uppermost NH on the five-membered ring is "7", counting counter-clockwise around this ring to the lower NH, which is "9".)
Uric acid was first isolated from kidney stones in 1776 by the Swedish chemist Carl Wilhelm Scheele. In 1882, the Ukrainian chemist Ivan Horbaczewski first synthesized uric acid by melting urea with glycine.
Solubility
In general, the water solubility of uric acid and its alkali metal and alkaline earth salts is rather low. All these salts exhibit greater solubility in hot water than cold, allowing for easy recrystallization. This low solubility is significant for the etiology of gout. The solubility of the acid and its salts in ethanol is very low or negligible. In ethanol/water mixtures, the solubilities are somewhere between the end values for pure ethanol and pure water.
The figures given indicate what mass of water is required to dissolve a unit mass of compound indicated. The lower the number the more soluble the substance in the said solvent.
Biology
The enzyme Xanthine oxidase catalyzes formation of uric acid from xanthine and hypoxanthine, which in turn are produced from other purines. Xanthine oxidase is a large enzyme whose active site consists of the metal molybdenum bound to sulfur and oxygen. Within cells, xanthine oxidase can exist as xanthine dehydrogenase and xanthine oxireductase, which has also been purified from bovine milk and spleen extracts. Uric acid is released in hypoxic conditions.
In humans and higher primates, uric acid (actually hydrogen urate ion) is the final oxidation (breakdown) product of purine metabolism and is excreted in urine. In most other mammals, the enzyme uricase further oxidizes uric acid to allantoin. The loss of uricase in higher primates parallels the similar loss of the ability to synthesize ascorbic acid, leading to the suggestion that urate may partially substitute for ascorbate in such species. Both uric acid and ascorbic acid are strong reducing agents (electron donors) and potent antioxidants. In humans, over half the antioxidant capacity of blood plasma comes from hydrogen urate ion.
The normal concentration range of uric acid (or hydrogen urate ion) in human blood is 25 to 80 mg/L for men and 15 to 60 mg/L for women (but see below for slightly different values). An individual can have serum values as high as 96 mg/L and not have gout. In humans, about 70% of daily uric acid disposal occurs via the kidneys, and in 5–25% of humans, impaired renal (kidney) excretion leads to hyperuricemia. Normal excretion of uric acid in the urine is 250 to 750 mg per day (concentration of 250 to 750 mg/L if one litre of urine is produced per day — higher than the solubility of uric acid because it is in the form of dissolved acid urates).
The Dalmatian dog has a genetic defect in uric acid uptake by the liver and kidneys, resulting in decreased conversion to allantoin, so this breed excretes uric acid, and not allantoin, in the urine.
In birds and reptiles, and in some desert dwelling mammals (e.g., the kangaroo rat), uric acid also is the end-product of purine metabolism, but it is excreted in feces as a dry mass. This involves a complex metabolic pathway that is energetically costly in comparison to processing of other nitrogenous wastes such as urea (from urea cycle) or ammonia, but has the advantages of reducing water loss and preventing dehydration.
Platynereis dumerilii, a marine polychaete worm, uses uric acid as a sexual pheromone released into the water by females during mating to induce males to release sperm.
Genetics
A proportion of people have mutations in the proteins responsible for the excretion of uric acid by the kidneys. Variants within a number of genes have so far been identified: SLC2A9; ABCG2; SLC17A1; SLC22A11; SLC22A12; SLC16A9; GCKR; LRRC16A; and PDZK1. SLC2A9 is known to transport both uric acid and fructose.
Medicine
In human blood plasma, the reference range of uric acid is typically 3.4–7.2 mg/dL (200–430 µmol/L) for men, and 2.4–6.1 mg/dL for women (140–360 µmol/L) – one milligram per decilitre (mg/dL) equals 59.48 micromoles/litre (µmol/L). However, blood test results should always be interpreted using the range provided by the laboratory that performed the test. Uric acid concentrations in blood plasma above and below the normal range are known as, respectively, hyperuricemia and hypouricemia. Likewise, uric acid concentrations in urine above and below normal are known as hyperuricosuria and hypouricosuria. Such abnormal concentrations of uric acid are not medical conditions, but are associated with a variety of medical conditions.
High uric acid
Hyperuricemia (high levels of uric acid) can lead to gout.
Causes of high uric acid
Gout
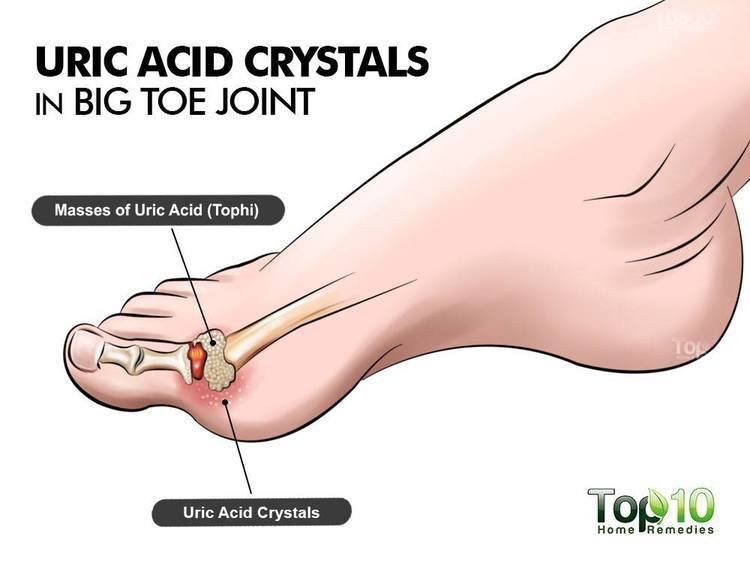
Excess serum accumulation of uric acid in the blood can lead to gout, which is a type of arthritis. This painful condition is the result of needle-like crystals of uric acid precipitating in joints, capillaries, skin, and other tissues. Kidney stones can also form through the process of formation and deposition of sodium urate microcrystals. Gout can occur where serum uric acid levels are as low as 6 mg/dL (~357 µmol/L), but an individual can have serum values as high as 9.6 mg/dL (~565 µmol/L) and not have gout.
In humans, purines are metabolized into uric acid which is then excreted in the urine. Consumption of some types of purine-rich foods, particularly meat and seafood, therefore increases the risk of gout. Patients with gout should avoid meats such as liver, kidney, and sweetbreads, and certain types of seafood including anchovies, herring, sardines, mussels, scallops, trout, haddock, mackerel and tuna. Moderate intake of purine-rich vegetables, however, is not associated with an increased risk of gout.
One treatment for gout in the 19th century was administration of lithium salts; lithium urate is more soluble. Today, inflammation during attacks is more commonly treated with NSAIDs, colchicine, or corticosteroids, and urate levels are managed with allopurinol. allopurinol, which weakly inhibits xanthine oxidase, is an analog of hypoxanthine that is hydroxylated by xanthine oxidoreductase at the 2-position to give oxipurinol. Oxipurinol has been supposed to bind tightly to the reduced molybdenum ion in the enzyme and, thus, inhibits uric acid synthesis.
Lesch-Nyhan syndrome
Lesch-Nyhan syndrome, an extremely rare inherited disorder, is also associated with very high serum uric acid levels. Spasticity, involuntary movement, and cognitive retardation as well as manifestations of gout are seen in cases of this syndrome.
Cardiovascular disease
Hyperuricemia may be associated with an increase in risk factors for cardiovascular disease.
Type 2 diabetes
The association of high serum uric acid with insulin resistance has been known since the early part of the 20th century, but the hypothesis that high serum uric acid is a risk factor for diabetes has long been a matter of debate. In fact, hyperuricemia was presumed to be a consequence of insulin resistance rather than its precursor. However, a prospective follow-up study showed high serum uric acid is associated with higher risk of type 2 diabetes, independent of obesity, dyslipidemia, and hypertension.
Metabolic syndrome
Hyperuricemia is associated with components of metabolic syndrome. A study has suggested fructose-induced hyperuricemia may play a pathogenic role in the metabolic syndrome. This is consistent with the increased consumption in recent decades of fructose-containing beverages (such as fruit juices and soft drinks sweetened with sugar and high-fructose corn syrup) and the epidemic of diabetes and obesity.
Uric acid stone formation
Saturation levels of uric acid in blood may result in one form of kidney stones when the urate crystallizes in the kidney. These uric acid stones are radiolucent and so do not appear on an abdominal plain X-ray, and thus their presence must be diagnosed by ultrasound for this reason or stone protocol CT. Very large stones may be detected on X-ray by their displacement of the surrounding kidney tissues.
Uric acid stones, which form in the absence of secondary causes such as chronic diarrhea, vigorous exercise, dehydration, and animal protein loading, are felt to be secondary to obesity and insulin resistance seen in metabolic syndrome. Increased dietary acid leads to increased endogenous acid production in the liver and muscles, which in turn leads to an increased acid load to the kidneys. This load is handled more poorly because of renal fat infiltration and insulin resistance, which are felt to impair ammonia excretion (a buffer). The urine is, therefore, quite acidic, and uric acid becomes insoluble, crystallizes and stones form. In addition, naturally present promoter and inhibitor factors may be affected. This explains the high prevalence of uric stones and unusually acidic urine seen in patients with type 2 diabetes. Uric acid crystals can also promote the formation of calcium oxalate stones, acting as "seed crystals" (heterogeneous nucleation).
Causes of low uric acid
Low uric acid (hypouricemia) can have numerous causes.
Low dietary zinc intakes cause lower uric acid levels. This effect can be even more pronounced in women taking oral contraceptive medication.
Xanthine oxidase (XO) is an iron–molybdenum enzyme, so people with iron deficiency (the most common cause of anemia in young women) or molybdenum deficiency can experience hypouricemia.
Xanthine oxidase loses its function and gains ascorbase function when some of the iron atoms in XO are replaced with copper atoms. In such cases, people with high copper/iron can experience hypouricemia and vitamin C deficiency, resulting in oxidative damage. Since estrogen increases the half-life of copper, people with very high estrogen levels and abundant blood loss during menstruation are likely to have high copper/iron and present with hypouricemia.
Sevelamer, a drug indicated for prevention of hyperphosphataemia in patients with chronic renal failure, can significantly reduce serum uric acid.
But the main cause of congenitally low uric acid, sometimes as low as zero, remains the molybdenum cofactor deficiency.
Multiple sclerosis
In one preliminary study, lower serum values of uric acid were somewhat associated with multiple sclerosis in which people with the disease had serum levels of ~194 µmol/L, people in relapse averaged ~160 µmol/L, and people in remission had ~230 µmol/L. Serum uric acid in healthy people was ~290 µmol/L.
Normalizing low uric acid
Correcting low or deficient zinc levels can help elevate serum uric acid. Inosine can be used to elevate uric acid levels. Zinc inhibits copper absorption, helping to reduce the high copper/iron in some people with hypouricemia. Iron supplements can ensure adequate iron reserves (ferritin above 25 ng/dl), also correcting the high copper/iron.
Oxidative stress
Uric acid may be a marker of oxidative stress, and may have a potential therapeutic role as an antioxidant. On the other hand, like other strong reducing substances such as ascorbate, uric acid can also act as a prooxidant. Thus, it is unclear whether elevated levels of uric acid in diseases associated with oxidative stress such as stroke and atherosclerosis are a protective response or a primary cause.
For example, some researchers propose hyperuricemia-induced oxidative stress is a cause of metabolic syndrome. On the other hand, plasma uric acid levels correlate with longevity in primates and other mammals. This is presumably a function of urate's antioxidant properties.