
ICD-9-CM 362.15, 448.0 MedlinePlus 003284 | ICD-10 G11.3, I78.0, M34.1 DiseasesDB 27395 MeSH D013684 | |
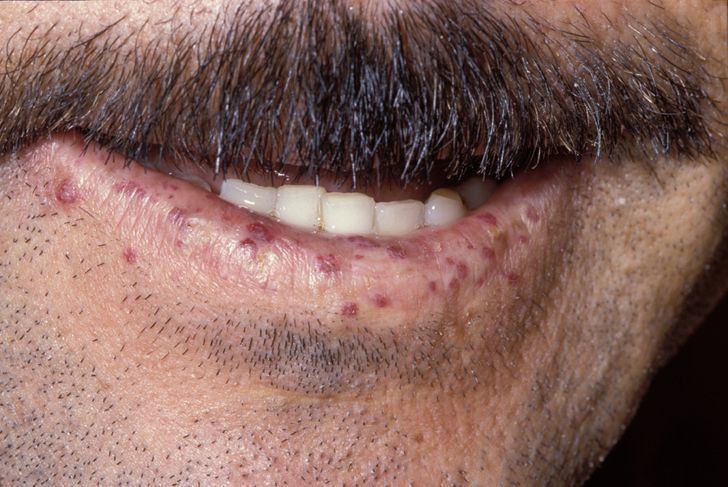 | ||
Telangiectasias /tɛlˌæn.dʒiː.ɛkˈteɪ.zi.ə/, also known as spider veins or angioectasias, are small dilated blood vessels near the surface of the skin or mucous membranes, measuring between 0.5 and 1 millimeter in diameter.
Contents
- Causes
- Congenital causes
- Acquired causes
- Venous hypertension
- Other acquired causes
- Treatment
- In popular culture
- References
These dilated blood vessels can develop anywhere on the body but are commonly seen on the face around the nose, cheeks, and chin. Dilated blood vessels can also develop on the legs, although when they occur on the legs, they often have underlying venous reflux or "hidden varicose veins" (see "Venous reflux" below). When found on the legs, they are found specifically on the upper thigh, below the knee joint, and around the ankles.
Many patients who suffer with spider veins seek the assistance of physicians who specialize in vein care or peripheral vascular disease. These physicians are called vascular surgeons or phlebologists. More recently, interventional radiologists have started treating venous problems.
Some telangiectasia are due to developmental abnormalities that can closely mimic the behaviour of benign vascular neoplasms. They may be composed of abnormal aggregations of arterioles, capillaries, or venules. Because telangiectasias are vascular lesions, they blanch when tested with diascopy.
Telangiectasia is a component of the CREST variant of scleroderma, also known today as limited scleroderma (CREST is an acronym that stands for calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia).
Causes
The causes of telangiectasia can be divided into congenital and acquired factors.
Congenital causes
Goldman states that "numerous inherited or congenital conditions display cutaneous telangiectasia". These include:
Acquired causes
Venous hypertension
In the past, people used to think that leg varicose veins or telangectasia were caused by high venous pressure or "venous hypertension". However it is now understood that venous reflux disease is usually the cause of these problems (see above for reference for "venous reflux".
Telangiectasia in the legs is often related to the presence of venous reflux within underlying varicose veins. Flow abnormalities within the medium-sized veins of the leg (reticular veins) can also lead to the development of telangiectasia. Factors that predispose to the development of varicose and telangiectatic leg veins include
Other acquired causes
Acquired telangiectasia, not related to other venous abnormalities, for example on the face and trunk, can be caused by factors such as
Treatment
Before any treatment of leg telangectasia (spider veins) is considered, it is essential to have duplex ultrasonography, the test that has replaced Doppler ultrasound. The reason for this is that there is a clear association between leg telangectasia (spider veins) and underlying venous reflux. Research has shown that 88-89% of women with telangectasia (spider veins) have refluxing reticular veins close, and 15% have incompetent perforator veins nearby. As such, it is essential to both find and treat underlying venous reflux before considering any treatment at all.
Sclerotherapy is the "gold standard" and is preferred over laser for eliminating telangiectasiae and smaller varicose leg veins. A sclerosant medication is injected into the diseased vein so it hardens and eventually shrinks away. Recent evidence with foam sclerotherapy shows that the foam containing the irritating sclerosant quickly appears in the patient's heart and lungs, and then in some cases travels through a patent foramen ovale to the brain. This has led to concerns about the safety of sclerotherapy for telangectasias and spider veins.
In some cases stroke and transient ischemic attacks have occurred after sclerotherapy. Varicose veins and reticular veins are often treated before treating telangiectasia, although treatment of these larger veins in advance of sclerotherapy for telangiectasia may not guarantee better results. Varicose veins can be treated with foam sclerotherapy, endovenous laser treatment, radiofrequency ablation, or open surgery. The biggest risk, however, seems to occur with sclerotherapy, especially in terms of systemic risk of DVT, pulmonary embolism, and stroke.
Other issues which arise with the use of sclerotherapy to treat spider veins are staining, shadowing, telangetatic matting, and ulceration. In addition, incompleteness of therapy is common, requiring multiple treatment sessions.
Telangiectasias on the face are often treated with a laser. Laser therapy uses a light beam that is pulsed onto the veins in order to seal them off, causing them to dissolve. These light-based treatments require adequate heating of the veins. These treatments can result in the destruction of sweat glands, and the risk increases with the number of treatments.
In popular culture
In spite of this condition being somewhat common in the populations of English speaking peoples, it is almost completely unknown in popular culture. It is mentioned (as t. langiatasis, when spoken) as "a condition that anyone can get" in Wodehouse Playhouse Series 1 : "Romance at Droitgate" (Spa) 30 April 1975.