
 | ||
The renin–angiotensin system (RAS) or the renin–angiotensin–aldosterone system (RAAS) is a hormone system that is involved in the regulation of the plasma sodium concentration and arterial blood pressure.
Contents
- Activation
- Cardiovascular effects
- Local renin angiotensin systems
- Fetal renin angiotensin system
- Clinical significance
- References
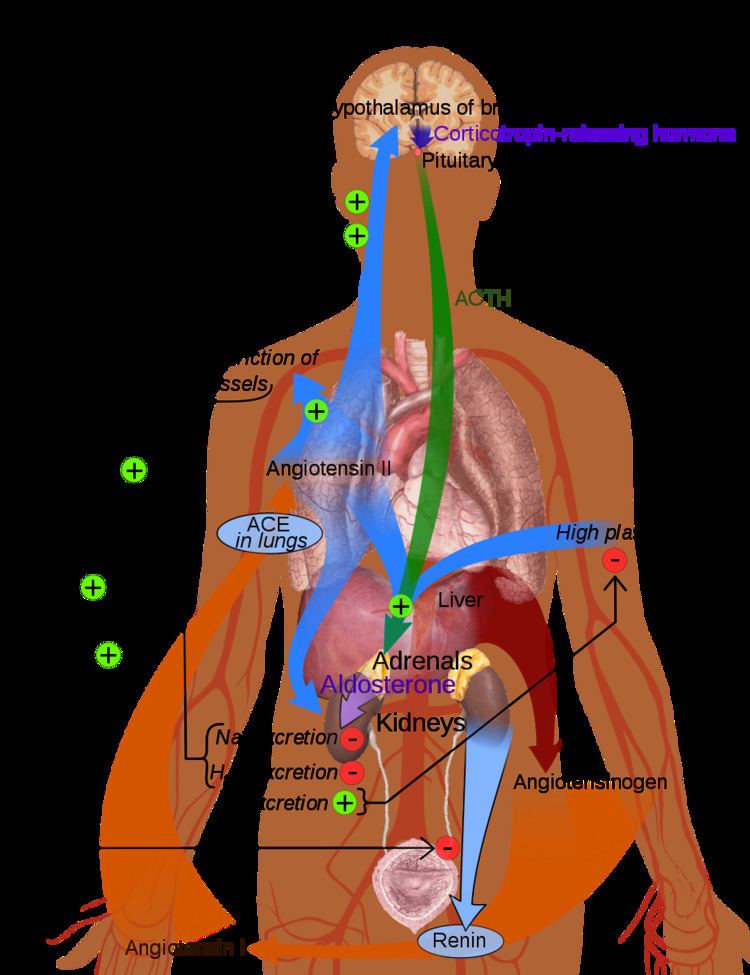
When the plasma sodium concentration is lower than normal or the renal blood flow is reduced, the juxtaglomerular cells in the kidneys convert prorenin (an intracellular protein) into renin, which is then secreted directly into the circulation. Plasma renin then cuts a short, 10 amino acid long, peptide off a plasma protein known as angiotensinogen. The short peptide is known as angiotensin I. Angiotensin I is then converted, by the removal of 2 amino acids, to form an octapeptide known as angiotensin II, by the enzyme angiotensin-converting enzyme (ACE) found in the endothelial cells of the capillaries throughout the body, within the lungs and the epithelial cells of the kidneys. Angiotensin II is a potent vaso-active peptide that causes arterioles to constrict, resulting in increased arterial blood pressure. Angiotensin II also stimulates the secretion of the hormone aldosterone from the adrenal cortex. Aldosterone causes the tubular epithelial cells of the kidneys to increase the reabsorption of sodium ions from the tubular fluid back into the blood, while at the same time causing them to excrete potassium ions into the tubular fluid which will become urine.
If the RAAS is abnormally active, blood pressure will be too high. There are many drugs that interrupt different steps in this system to lower blood pressure. These drugs are one of the primary ways to control high blood pressure (hypertension), heart failure, kidney failure, and harmful effects of diabetes.
Activation
The system can be activated when there is a loss of blood volume or a drop in blood pressure (such as in hemorrhage or dehydration). This loss of pressure is interpreted by baroreceptors in the carotid sinus. In alternative fashion, a decrease in the filtrate NaCl concentration and/or decreased filtrate flow rate will stimulate the macula densa to signal the juxtaglomerular cells to release renin.
- If the perfusion of the juxtaglomerular apparatus in the kidney's macula densa decreases, then the juxtaglomerular cells (granular cells, modified pericytes in the glomerular capillary) release the enzyme renin.
- Renin cleaves a decapeptide from a plasma α-2-globulin called angiotensinogen. The 10 amino acid long peptide is known as angiotensin I.
- Angiotensin I is then converted to angiotensin II by angiotensin-converting enzyme (ACE), which is thought to be found mainly in lung capillaries. One study in 1992 found ACE in all blood vessel endothelial cells.
- Angiotensin II is the major bioactive product of the renin-angiotensin system, binding to receptors on intraglomerular mesangial cells, causing these cells to contract along with systemic blood vessels. Angiotensin II is a potent vasoconstrictor, 40X more potent than epinephrine. Angiotensin II also acts on the adrenal cortex culminating in the release of aldosterone from the zona glomerulosa. Angiotensin II acts as an endocrine, autocrine/paracrine, and intracrine hormone.
Cardiovascular effects
Further reading: Angiotensin#Effects and Aldosterone#FunctionIt is believed that angiotensin I may have some minor activity, but angiotensin II is the major bio-active product. Angiotensin II has a variety of effects on the body:
/H+
exchangers located on the apical membranes (faces the tubular lumen) of cells in the proximal tubule and thick ascending limb of the loop of Henle in addition to Na+
channels in the collecting ducts. This will ultimately lead to increased sodium reabsorption.
The prevention of sodium losses via the urine, and the correction of any deficit by consuming salt act together to increase blood pressure. These actions are opposed by atrial natriuretic peptide (ANP) which is secreted from the atria of the heart in response to stretch caused by an excessive blood volume.
Local renin-angiotensin systems
Locally expressed renin-angiotensin systems have been found in a number of tissues, including the kidneys, adrenal glands, the heart, vasculature and nervous system, and have a variety of functions, including local cardiovascular regulation, in association or independently of the systemic renin-angiotensin system, as well as non-cardiovascular functions. Outside the kidneys, renin is predominantly picked up from the circulation but may be secreted locally in some tissues; its precursor prorenin is highly expressed in tissues and more than half of circulating prorenin is of extrarenal origin, but its physiological role besides serving as precursor to renin is still unclear. Outside the liver, angiotensinogen is picked up from the circulation or expressed locally in some tissues; with renin they form angiotensin I, and locally expressed angiotensin-converting enzyme, chymase or other enzymes can transform it into angiotensin II. This process can be intracellular or interstitial.
In the adrenal glands, it is likely involved in the paracrine regulation of aldosterone secretion, in the heart and vasculature, it may be involved in remodeling or vascular tone, and in the brain where it is largely independent of the circulatory RAS, it may be involved in local blood pressure regulation. In addition, both the central and peripheral nervous systems can use angiotensin for sympathetic neurotransmision. Other places of expression include the reproductive system, the skin and digestive organs. Medications aimed at the systemic system may affect the expression of those local systems, beneficially or adversely.
Fetal renin-angiotensin system
In the fetus, the renin-angiotensin system is predominantly a sodium-losing system, as angiotensin II has little or no effect on aldosterone levels. Renin levels are high in the fetus, while angiotensin II levels are significantly lower; this is due to the limited pulmonary blood flow, preventing ACE (found predominantly in the pulmonary circulation) from having its maximum effect.