
EC number 3.4.15.1 ExPASy NiceZyme view | CAS number 9015-82-1 | |
 | ||
How do drugs work angiotensin converting enzyme inhibitors ace inhibitors
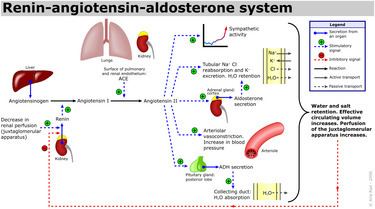
Angiotensin-converting enzyme (EC 3.4.15.1), or ACE, is a central component of the renin-angiotensin system (RAS), which controls blood pressure by regulating the volume of fluids in the body. It converts the hormone angiotensin I to the active vasoconstrictor angiotensin II. Therefore, ACE indirectly increases blood pressure by causing blood vessels to constrict. ACE inhibitors are widely used as pharmaceutical drugs for treatment of cardiovascular diseases.
Contents
- How do drugs work angiotensin converting enzyme inhibitors ace inhibitors
- Function
- Mechanism
- Genetics
- Disease relevance
- Pathology
- Influence on athletic performance
- References
The enzyme was discovered by Leonard T. Skeggs Jr. in 1956. It is located mainly in the capillaries of the lungs but can also be found in endothelial and kidney epithelial cells.
Other less known functions of ACE are degradation of bradykinin and amyloid beta-protein.
Function
ACE hydrolyzes peptides by the removal of a dipeptide from the C-terminus. Likewise it converts the inactive decapeptide angiotensin I to the octapeptide angiotensin II by removing the dipeptide His-Leu.
Angiotensin II is potent vasoconstrictor in a substrate concentration-dependent manner. Angiotensin II binds to the type 1 angiotensin II receptor (AT1), which sets off a number of actions that result in vasoconstriction and therefore increased blood pressure.
ACE is also part of the kinin-kallikrein system where it degrades bradykinin, a potent vasodilator, and other vasoactive peptides.
Kininase II is the same as angiotensin-converting enzyme. Thus, the same enzyme (ACE) that generates a vasoconstrictor (ANG II) also disposes of vasodilators (bradykinin).
Mechanism
ACE is a zinc metalloenzyme. The zinc ion is essential to its activity, since it directly participates in the catalysis of the peptide hydrolysis. Therefore, ACE can be inhibited by metal-chelating agents.
The E384 residue was found to have a dual function. First it acts as a general base to activate water as a nucleophile. Then it acts as a general acid to cleave the C-N bond.
The function of the chloride ion is very complex and is highly debated. The anion activation by chloride is a characteristic feature of ACE. It was experimentally determined that the activation of hydrolysis by chloride is highly dependent on the substrate. While it increases hydrolysis rates for e.g. Hip-His-Leu it inhibits hydrolysis of other substrates like Hip-Ala-Pro. Under physiological conditions the enzyme reaches about 60% of its maximal activity toward angiotensin I while it reaches its full activity toward bradykinin. It is therefore assumed that the function of the anion activation in ACE provides high substrate specificity. Other theories say that the chloride might simply stabilize the overall structure of the enzyme.
Genetics
The ACE gene, ACE, encodes two isozymes. The somatic isozyme is expressed in many tissues, mainly in the lung, including vascular endothelial cells, epithelial kidney cells, and testicular Leydig cells, whereas the germinal is expressed only in sperm. Brain tissue has ACE enzyme, which takes part in local RAS and converts Aβ42 (which aggregates into plaques) to Aβ40 (which is thought to be less toxic) forms of beta amyloid. The latter is predominantly a function of N domain portion on the ACE enzyme. ACE inhibitors that cross the blood–brain barrier and have preferentially selected N-terminal activity may therefore cause accumulation of Aβ42 and progression of dementia.
Disease relevance
ACE inhibitors are widely used as pharmaceutical drugs in the treatment of conditions such as high blood pressure, heart failure, diabetic nephropathy, and type 2 diabetes mellitus.
ACE inhibitors inhibit ACE competitively. That results in the decreased formation of angiotensin II and decreased metabolism of bradykinin, which leads to systematic dilation of the arteries and veins and a decrease in arterial blood pressure. In addition, inhibiting angiotensin II formation diminishes angiotensin II-mediated aldosterone secretion from the adrenal cortex, leading to a decrease in water and sodium reabsorption and a reduction in extracellular volume.
ACE's effect on Alzheimer's disease is still highly debated. Alzheimer patients usually show higher ACE levels in their brain. Some studies suggest that ACE inhibitors that are able to pass the blood-brain-barrier (BBB) could enhance the activity of major amyloid-beta peptide degrading enzymes like neprilysin in the brain resulting in a slower development of Alzheimer's disease. More recent research suggests that ACE inhibitors can reduce risk of Alzheimer's disease in the absence of apolipoprotein E4 alleles (ApoE4), but will have no affect in ApoE4- carriers. Another more recent hypothesis is that higher levels of ACE can prevent Alzheimer's. It is assumed that ACE can degrade beta-amyloid in brain blood vessels and therefore help prevent the digression of the disease.
Pathology
Influence on athletic performance
Studies have shown that different genotypes of angiotensin converting enzyme can lead to varying influence on athletic performance. ACE I/D polymorphism consists of either an insertion (I) or absence (D) of a 287 base pair alanine sequence in intron 16 of the gene. People carrying the I-allele usually have lower ACE levels while people carrying the D-allele have higher ACE levels.
People carrying the D-allele are associated with higher ACE levels that cause higher levels of angiotensin II. During physical exercise the blood pressure of D-allele carriers will therefore increase sooner than for I-allele carriers. This results in a lower maximal heart rate and lower maximum oxygen uptake (VO2max). Therefore, D-allele carriers have a 10% increased risk of cardiovascular diseases. Furthermore, the D-allele is associated with a greater increase in left ventricular growth in response to training compared to the I-allele. On the other hand, I-allele carriers usually show an increased maximal heart rate due to lower ACE levels, higher maximum oxygen uptake and therefore show an enhanced endurance performance.
The I allele is found with increased frequency in elite distance runners, rowers and cyclists. Short distance swimmers show a higher occurrence of D-allele carriers in their specific discipline, since their discipline relies more on strength than endurance.