
Entrez 4878 | Ensembl ENSG00000175206 | |
 | ||
Aliases NPPA, ANF, ANP, ATFB6, ATRST2, CDD, CDD-ANF, CDP, PND, Atrial natriuretic peptide, natriuretic peptide A External IDs OMIM: 108780 MGI: 97367 HomoloGene: 4498 GeneCards: NPPA | ||
Atrial natriuretic peptide (ANP), also called atrial natriuretic factor (ANF), atrial natriuretic hormone (ANH), cardionatrine, cardiodilatin (CDD), or atriopeptin, is a powerful vasodilator, and a protein (polypeptide) hormone secreted by heart muscle cells. It is involved in the homeostatic control of body water, sodium, potassium and fat (adipose tissue). It is released by muscle cells in the upper chambers (atria) of the heart (atrial myocytes) in response to high blood volume. ANP acts to reduce the water, sodium and adipose loads on the circulatory system, thereby reducing blood pressure. ANP has exactly the opposite function of the aldosterone secreted by the zona glomerulosa in regard to its effect on sodium in the kidney – that is, aldosterone stimulates sodium retention and ANP generates sodium loss.
Contents
Discovery
ANP was discovered in the early 1980s. de Bold and colleagues in Kingston, Ontario, Canada found that rat atrial extracts contained a substance that increased salt and urine output in the kidney. Later, the substance was purified from the heart by several groups and named ANF or ANP.
Structure
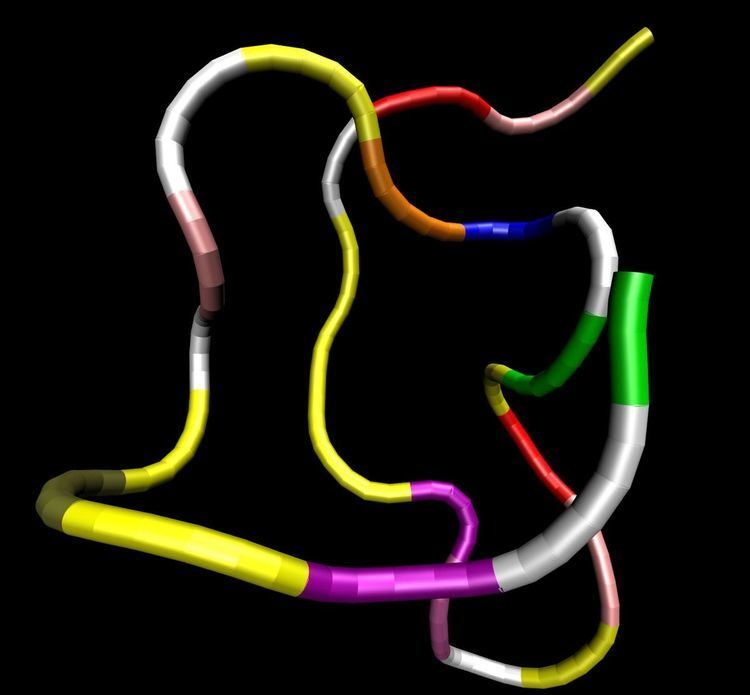
ANP is a 28-amino acid peptide with a 17-amino acid ring in the middle of the molecule. The ring is formed by a disulfide bond between two cysteine residues at positions 7 and 23. ANP is closely related to BNP (brain natriuretic peptide) and CNP (C-type natriuretic peptide), which all share a similar amino acid ring structure.
Production
Human ANP is encoded by the NPPA gene on the short arm of chromosome 1, which has 3 exons and 2 introns. The gene is expressed primarily in cardiac myocytes. Lower levels of NPPA expression are found in other tissues such as the brain, kidney, lung, uterus and placenta.
In cardiac myocytes, ANP is made as a precursor form, i.e. prepro-ANP, a polypeptide of 151 amino acids. After the signal peptide is removed in the endoplasmic reticulum, the 126-amino-acid pro-ANP is stored in the intracellular granules. When the cells are stimulated, pro-ANP is released and converted to the 28-amino-acid C-terminal mature ANP on the cell surface by the cardiac transmembrane serine protease corin.
ANP is secreted in response to:
Receptors
Three types of atrial natriuretic peptide receptors have been identified on which natriuretic peptides act. They are all cell surface receptors and designated:
NPR-A and NPR-B have a single membrane-spanning segment with an extracellular domain that binds the ligand. The intracellular domain maintains two consensus catalytic domains for guanylyl cyclase activity. Binding of a natriuretic peptide induces a conformational change in the receptor that causes receptor dimerization and activation.
The binding of ANP to its receptor causes the conversion of GTP to cGMP and raises intracellular cGMP. As a consequence, cGMP activates a cGMP-dependent kinase (PKG or cGK) that phosphorylates proteins at specific serine and threonine residues. In the medullary collecting duct, the cGMP generated in response to ANP may act not only through PKG but also via direct modulation of ion channels.
NPR-C functions mainly as a clearance receptor by binding and sequestering ANP from the circulation. All natriuretic peptides are bound by the NPR-C.
ANP and brain natriuretic peptide bind and activate GC-A, whereas CNP binds and activates GC-B.
Physiological effects
ANP binds to a specific set of receptors – ANP receptors. Receptor-agonist binding causes a reduction in blood volume and, therefore, a reduction in cardiac output and systemic blood pressure. Lipolysis is increased and renal sodium reabsorption is decreased. The overall effect of ANP on the body is to counter increases in blood pressure and volume caused by the renin-angiotensin system.
Renal
Adrenal
Vascular
Relaxes vascular smooth muscle in arterioles and venules by:
Promotes uterine spiral artery remodeling, which is important for preventing pregnancy-induced hypertension.
Cardiac
It may be associated with isolated atrial amyloidosis.
Adipose tissue
Degradation
Regulation of the effects of ANP is achieved through gradual degradation of the peptide by the enzyme neutral endopeptidase (NEP). Recently, NEP inhibitors have been developed; however they have not yet been licensed. They may be clinically useful in treating congestive heart disease.
Biomarker
Fragments derived from the ANP precursor, including the signal peptide, N-terminal pro-ANP and ANP, have been detected in human blood. ANP and related peptides are used as biomarkers for cardiovascular diseases such as stroke, coronary artery disease, myocardial infarction and heart failure.
Large amounts of ANP secretion has been noted to cause electrolyte disturbances (hyponatremia) and polyuria. These indications can be a marker of a large atrial myxoma.
Therapeutic use
Recombinant human ANP has been approved in Japan to treat patients with heart failure.
Other natriuretic factors
In addition to the mammalian natriuretic peptides (ANP, BNP, CNP), other natriuretic peptides with similar structure and properties have been isolated elsewhere in the animal kingdom. Tervonen (1998) described a salmon natriuretic peptide known as salmon cardiac peptide, while dendroaspis natriuretic peptide (DNP) can be found in the venom of the green mamba, a species of African snake.
Pharmacological modulation
Neutral endopeptidase (NEP) also known as neprilysin is the enzyme that metabolizes natriuretic peptides. Several inhibitors of NEP are currently being developed to treat disorders ranging from hypertension to heart failure. Most of them are dual inhibitors (NEP and ACE). In 2014, PARADIGM-HF study was published in NEJM. This study considered as a landmark study in treatment of heart failure. The study was double blinded; compared LCZ696 versus enalapril in patients with heart failure. The study showed lower all cause mortality, cardiovascular mortality and hospitalization in LCZ696 arm. Omapatrilat (dual inhibitor of NEP and angiotensin-converting enzyme) developed by BMS did not receive FDA approval due to angioedema safety concerns. Other dual inhibitors of NEP with ACE/angiotensin receptor are (in 2003) being developed by pharmaceutical companies.