
ICD-9-CM 434.91 eMedicine pmr/63 | ICD-10 G46.5-G46.7 DiseasesDB 31186 MeSH D020520 | |
 | ||
Lacunar stroke or lacunar infarct (LACI) is the most common type of stroke, and results from occlusion of small penetrating arteries that provide blood to the brain's deep structures. Patients who present with symptoms of a lacunar stroke, but who have not yet had diagnostic imaging performed, may be described as suffering from lacunar stroke syndrome (LACS).
Contents
- Signs and symptoms
- Silent lacunar infarction
- Pathophysiology
- Treatment and prognosis
- Epidemiology
- References
Much of the current knowledge of lacunar strokes comes from C. Miller Fisher's cadaver dissections of post-mortem stroke patients. He observed "lacunae" (empty spaces) in the deep brain structures after occlusion of 200–800 μm penetrating arteries and connected them with five classic syndromes. These syndromes are still noted today, though lacunar infarcts are diagnosed based on clinical judgment and radiologic imaging.
Signs and symptoms
Each of the 5 classical lacunar syndromes has a relatively distinct symptom complex. Symptoms may occur suddenly, progressively, or in a fluctuating (e.g., the capsular warning syndrome) manner. Occasionally, cortical infarcts and intracranial hemorrhages can mimic lacunar infarcts, but true cortical infarct signs (aphasia, visuospatial neglect, gaze deviation, and visual field defects) are always absent. The 5 classic syndromes are as follows:
Silent lacunar infarction
A silent lacunar infarction (SLI) is one type of silent stroke which usually shows no identifiable outward symptoms thus the term "silent". Individuals who suffer a SLI are often completely unaware they have suffered a stroke. This type of stroke often causes lesions in the surrounding brain tissue that are visibly detected via neuroimaging techniques such as MRI and computerized axial tomography (CT scan). Silent strokes, including silent lacunar infarctions, have been shown to be much more common than previously thought, with an estimated prevalence rate of eleven million per year in the United States. Approximately 10% of these silent strokes are silent lacunar infarctions. While dubbed "silent" due to the immediate lack of classic stroke symptoms, SLIs can cause damage to the surrounding brain tissue (lesions) and can affect various aspects of a persons mood, personality, and cognitive functioning. A SLI or any type of silent stroke places an individual at greater risk for future major stroke.
Pathophysiology
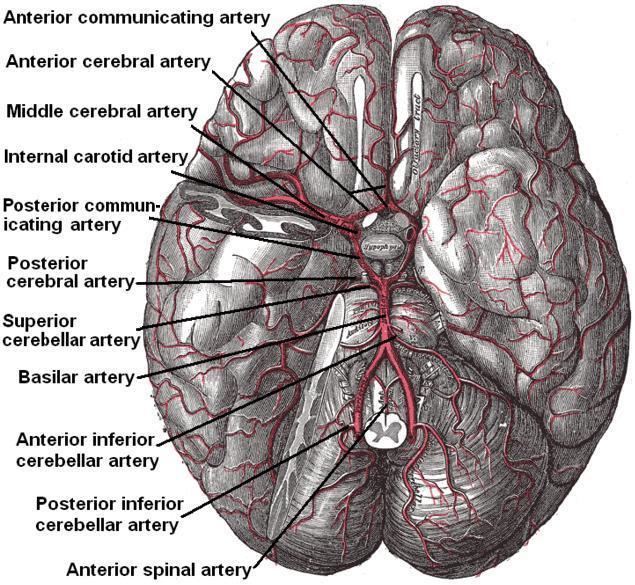
Lacunes are caused by occlusion of a single deep penetrating artery that arises directly from the constituents of the Circle of Willis, cerebellar arteries, and basilar artery. The corresponding lesions occur in the deep nuclei of the brain (37% putamen, 14% thalamus, and 10% caudate) as well as the pons (16%) or the posterior limb of the internal capsule (10%). They occur less commonly in the deep cerebral white matter, the anterior limb of the internal capsule, and the cerebellum.
The two proposed mechanisms are microatheroma and lipohyalinosis. At the beginning, lipohyalinosis was thought to be the main small vessel pathology, but microatheroma now is thought to be the most common mechanism of arterial occlusion (or stenosis). Occasionally, atheroma in the parent artery blocks the orifice of the penetrating artery (luminal atheroma), or atheroma involves the origin of the penetrating artery (junctional atheroma). Alternatively, hypoperfusion is believed to be the mechanism when there is stenosis of the penetrating artery. When no evidence of small vessel disease is found on histologic examination, an embolic cause is assumed, either artery-to-artery embolism or cardioembolism. In one recent series, 25% of patients with clinical radiologically defined lacunes had a potential cardiac cause for their strokes.
Advanced age, chronic hypertension, smoking and diabetes mellitus are risk factors. It is unclear whether there is an association with alcohol consumption, elevated cholesterol, or history of prior stroke. Lacunar strokes may result from carotid artery pathology or microemboli from the heart as in atrial fibrillation. Patients often recover well, but if there is enough white matter disease from lacunar pathology, one can see a subcortical dementia such as Binswanger disease.
Treatment and prognosis
Typically, tissue plasminogen activator may be administered within three to four-and-a-half hours of stroke onset if the patient is without contraindications (i.e. a bleeding diathesis such as recent major surgery or cancer with brain metastases). High dose aspirin can be given within 48 hours. For long term prevention of recurrence, medical regimens are typically aimed towards correcting the underlying risk factors for lacunar infarcts such as hypertension, diabetes mellitus and cigarette smoking. Anticoagulants such as heparin and warfarin have shown no benefit over aspirin with regards to five year survival.
Patients who suffer lacunar strokes have a greater chance of surviving beyond thirty days (96%) than those with other types of stroke (85%), and better survival beyond a year (87% versus 65-70%). Between 70% and 80% are functionally independent at 1 year, compared with fewer than 50% otherwise.
Physiotherapy interventions are used in the rehabilitation of lacunar stroke. A physiotherapy program will improve joint range of motion of the paretic limb using passive range of motion exercises. When increases in activity are tolerated, and stability improvements are made, patients will progress from rolling to side-lying, to standing (with progressions to prone, quadruped, bridging, long-sitting and kneeling for example) and learn to transfer safely (from their bed to a chair or from a wheel chair to a car for example). Assistance and ambulation aids are used as required as the patient begins walking and lessened as function increases. Furthermore, splints and braces can be used to support limbs and joints to prevent complications such as contractures and spasticity. The rehabilitation healthcare team should also educate the patient and their family on common stroke symptoms and how to manage an onset of stroke. Continuing follow-up with a physician is essential so that the physician may monitor medication dosage and risk factors.
Epidemiology
It is estimated that lacunar infarcts account for 25% of all ischemic strokes, with an annual incidence of approximately 15 per 100,000 people. They may be more frequent in men and in people of African, Mexican, and Hong Kong Chinese descent.