
Specialty emergency medicine ICD-9-CM 430-432, 850-854 eMedicine neuro/177 | ICD-10 I60.0-I62, S06 DiseasesDB 6870 MeSH D020300 | |
 | ||
Intracranial hemorrhage (ICH), also known as intracranial bleed is bleeding within the skull. It includes intracerebral bleeds (intraventricular bleeds and intraparenchymal bleeds), subarachnoid bleeds, epidural bleeds, and subdural bleeds.
Contents
Intracerebral bleeding affects 2.5 per 10,000 people each year.
Signs and symptoms
Intracranial hemorrhage is a serious medical emergency because the buildup of blood within the skull can lead to increases in intracranial pressure, which can crush delicate brain tissue or limit its blood supply. Severe increases in intracranial pressure (ICP) can cause brain herniation, in which parts of the brain are squeezed past structures in the skull.
Causes
Intracranial bleeding occurs when a blood vessel within the skull is ruptured or leaks. It can result from physical trauma (as occurs in head injury) or nontraumatic causes (as occurs in hemorrhagic stroke) such as a ruptured aneurysm. Anticoagulant therapy, as well as disorders with blood clotting can heighten the risk that an intracranial hemorrhage will occur.
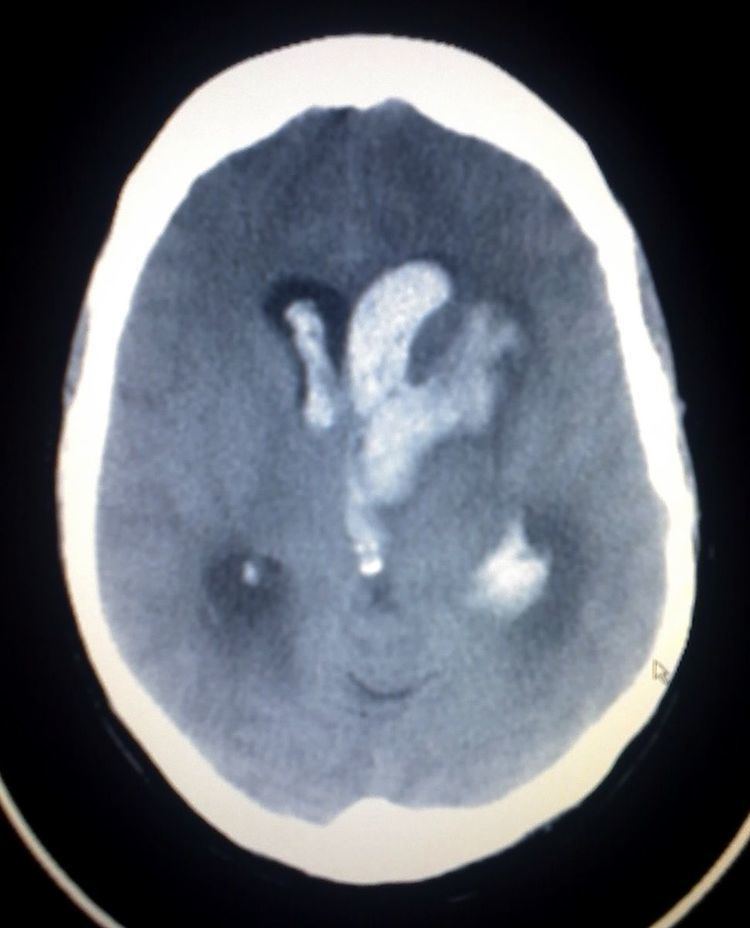
Diagnosis
CT scan (computed tomography) is the definitive tool for accurate diagnosis of an intracranial hemorrhage. In difficult cases, a 3T-MRI scan can also be used.
When ICP is increased the heart rate may be decreased.
Classification
Types of intracranial hemorrhage are roughly grouped into intra-axial and extra-axial. The hemorrhage is considered a focal brain injury; that is, it occurs in a localized spot rather than causing diffuse damage over a wider area.
Intra-axial bleed
Intra-axial hemorrhage is bleeding within the brain itself, or cerebral hemorrhage. This category includes intraparenchymal hemorrhage, or bleeding within the brain tissue, and intraventricular hemorrhage, bleeding within the brain's ventricles (particularly of premature infants). Intra-axial hemorrhages are more dangerous and harder to treat than extra-axial bleeds.
Extra-axial bleed
Extra-axial hemorrhage, bleeding that occurs within the skull but outside of the brain tissue, falls into three subtypes:
Epidural hematoma
Epidural hematoma (EDH) is a rapidly accumulating hematoma between the dura mater and the cranium. These patients have a history of head trauma with loss of consciousness, then a lucid period, followed by loss of consciousness. Clinical onset occurs over minutes to hours. Many of these injuries are associated with lacerations of the middle meningeal artery. A "lenticular", or convex, lens-shaped extracerebral hemorrhage that does not cross suture lines will likely be visible on a CT scan of the head. Although death is a potential complication, the prognosis is good when this injury is recognized and treated.
Subdural hematoma
Subdural hematoma occurs when there is tearing of the bridging vein between the cerebral cortex and a draining venous sinus. At times they may be caused by arterial lacerations on the brain surface. Acute subdural hematomas are usually associated with cerebral cortex injury as well and hence the prognosis is not as good as extra dural hematomas. Clinical features depend on the site of injury and severity of injury. Patients may have a history of loss of consciousness but they recover and do not relapse. Clinical onset occurs over hours. A crescent shaped hemorrhage compressing the brain that does cross suture lines will be noted on CT of the head. Craniotomy and surgical evacuation is required if there is significant pressure effect on the brain.Complications include focal neurologic deficits depending on the site of hematoma and brain injury, increased intra cranial pressure leading to herniation of brain and ischemia due to reduced blood supply and seizures.
Subarachnoid hemorrhage
A subarachnoid hemorrhage is bleeding into the subarachnoid space—the area between the arachnoid membrane and the pia mater surrounding the brain. Besides from head injury, it may occur spontaneously, usually from a ruptured cerebral aneurysm. Symptoms of SAH include a severe headache with a rapid onset ("thunderclap headache"), vomiting, confusion or a lowered level of consciousness, and sometimes seizures. The diagnosis is generally confirmed with a CT scan of the head, or occasionally by lumbar puncture. Treatment is by prompt neurosurgery or radiologically guided interventions with medications and other treatments to help prevent recurrence of the bleeding and complications. Since the 1990s, many aneurysms are treated by a minimal invasive procedure called "coiling", which is carried out by instrumentation through large blood vessels. However, this procedure has higher recurrence rates than the more invasive craniotomy with clipping.