
 | ||
Infant mortality refers to deaths of young children, typically those less than one year of age. It is measured by the infant mortality rate (IMR), which is the number of deaths of children under one year of age per 1000 live births. The Under-Five Mortality Rate is also an important statistic considering the Infant Mortality Rate has a strict limit on focusing on children only under one year of age.
Contents
- Classification
- Causes
- Medical
- Low birth weight
- Sudden infant death syndrome
- Malnutrition
- Infectious diseases
- Environmental
- Socio economic factors
- War
- Medicine and biology
- Economics
- Cultural
- Gender favoritism
- Birth spacing
- Education
- Prevention
- Public health
- Medical treatments
- Cultural changes
- EconomicSocial policies
- Differences in measurement
- Europe and America
- Russia
- Brazil
- Global trends
- In the United States
- African American Infant Mortality in the United States
- History
- Other meanings
- References
Premature birth is the biggest contributor to the IMR. Other leading causes of infant mortality are birth asphyxia, pneumonia, term birth complications, neonatal infection, diarrhea, malaria, measles and malnutrition. One of the most common preventable causes of infant mortality is smoking during pregnancy. Many factors contribute to infant mortality, such as the mother's level of education, environmental conditions, and political and medical infrastructure. Improving sanitation, access to clean drinking water, immunization against infectious diseases, and other public health measures can help reduce high rates of infant mortality.
Child mortality is the death of a child before the child's fifth birthday, measured as the Under-5 Child Mortality Rate (U5MR). National statistics sometimes group these two mortality rates together. Globally, ten million infants and children die each year before their fifth birthday; 99% of these deaths occur in developing nations.
Infant mortality rate was an indicator used to monitor progress towards the Fourth Goal of the Millennium Development Goals of the United Nations for the year 2015. It is now a target in the Sustainable Development Goals for Goal Number 3 ("Ensure healthy lives and promote well-being for all at all ages").
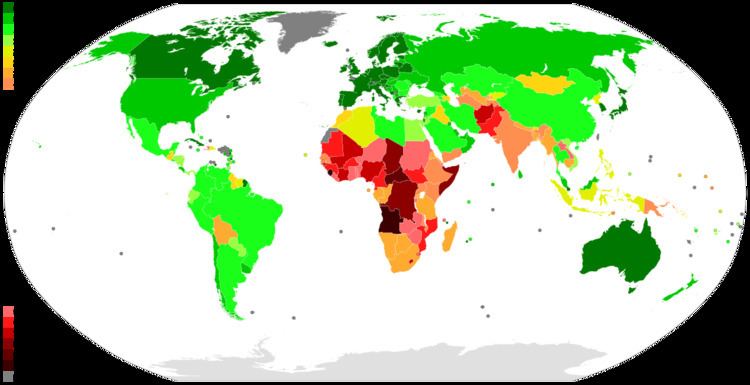
Throughout the world, Infant Mortality Rate (IMR) fluctuates drastically, and according to Biotechnology and Health Sciences, education and life expectancy in the country is the leading indicator of IMR. This study was conducted across 135 countries over the course of 11 years with Africa having the highest Infant Mortality Rate of any other region studied with 68 deaths per 1,000 live births.
Classification
Infant mortality rate (IMR) is the number of deaths of children less than one year of age per 1000 live births. The rate for a given region is the number of children dying under one year of age, divided by the number of live births during the year, multiplied by 1,000.
Forms of infant mortality:
Causes
Causes of infant mortality directly lead to the death. Environmental and social barriers prevent access to basic medical resources and thus contribute to an increasing infant mortality rate; 99% of infant deaths occur in developing countries, and 86% of these deaths are due to infections, premature births, complications during delivery, and perinatal asphyxia and birth injuries. Greatest percentage reduction of infant mortality occurs in countries that already have low rates of infant mortality. Common causes are preventable with low-cost measures. In the United States, a primary determinant of infant mortality risk is infant birth weight with lower birth weights increasing the risk of infant mortality. The determinants of low birth weight include socio-economic, psychological, behavioral and environmental factors.
Medical
Causes of infant mortality that are related to medical conditions include: low birth weight, sudden infant death syndrome, malnutrition and infectious diseases, including neglected tropical diseases.
Low birth weight
Low birth weight makes up 60–80% of the infant mortality rate in developing countries. The New England Journal of Medicine stated that "The lowest mortality rates occur among infants weighing 3,000 to 3,500 g (6.6 to 7.7 lb). For infants born weighing 2,500 g (5.5 lb) or less, the mortality rate rapidly increases with decreasing weight, and most of the infants weighing 1,000 g (2.2 lb) or less die. As compared with normal-birth-weight infants, those with low weight at birth are almost 40 times more likely to die in the neonatal period; for infants with very low weight at birth the relative risk of neonatal death is almost 200 times greater." Infant mortality due to low birth weight is usually a direct cause stemming from other medical complications such as preterm birth, poor maternal nutritional status, lack of prenatal care, maternal sickness during pregnancy, and an unhygienic home environments. Along with birth weight, period of gestation makes up the two most important predictors of an infant's chances of survival and their overall health.
According to the New England Journal of Medicine, "in the past two decades, the infant mortality rate (deaths under one year of age per thousand live births) in the United States has declined sharply." Low birth weights from African American mothers remain twice as high as that of white women. LBW may be the leading cause of infant deaths, and it is greatly preventable. Although it is preventable, the solutions may not be the easiest but effective programs to help prevent LBW are a combination of health care, education, environment, mental modification and public policy, influencing a culture supporting lifestyle. Preterm birth is the leading cause of newborn deaths worldwide. Even though America excels past many other countries in the care and saving of premature infants, the percentage of American woman who deliver prematurely is comparable to those in developing countries. Reasons for this include teenage pregnancy, increase in pregnant mothers over the age of thirty-five, increase in the use of in-vitro fertilization which increases the risk of multiple births, obesity and diabetes. Also, women who do not have access to health care are less likely to visit a doctor, therefore increasing their risk of delivering prematurely.
Sudden infant death syndrome
Thousands of infant deaths per year are classified as Sudden infant death syndrome (SIDS). According to the Mayo Clinic, SIDS is the unexplained death, usually during sleep, of a seemingly healthy baby. Although the direct cause of SIDS remains unknown, many doctors believe that there are several factors that put babies at an increased risk of SIDS, including: babies sleeping on their stomachs, exposure to cigarette smoke in the womb or after birth, sleeping in bed with parents, premature birth, being a twin or triplet, being born to a teen mother, and also living in poverty settings. Although the cause is unknown and currently cannot be explained, doctors have come to the conclusion that SIDS is most likely to occur between 2 and 4 months and most deaths occur in the winter time. Recommended precautions include ensuring that infants sleep on their backs, controlling the temperature of the bedroom, employing a crib without toys or excess bedding, and breastfeeding.
Malnutrition
Malnutrition frequently accompanies these diseases, and is a primary factor contributing to the complications of both diarrhea and pneumonia, although the causal links and mechanisms remain unclear. Factors other nutrition also influence the incidence of diarrhea, including socioeconomic status, disruption of traditional lifestyles, access to clean water and sanitation facilities, age and breastfeeding status.
Protein energy malnutrition and micronutrient deficiency are two reasons for stunted growth in children under five years old in the least developed countries. Malnutrition leads to diarrhea and dehydration, and ultimately death. Millions of women in developing countries are stunted due to a history of childhood malnutrition. Women's bodies are thus underdeveloped, and their chances of surviving childbirth decrease. Due to underdeveloped bodies, the probability of an obstructed pregnancy increases. Protein-energy deficiency results in low-quality breastmilk that provides less energy and other nutrition.
Vitamin A deficiency can lead to stunted growth, blindness, and increased mortality due to the lack of nutrients in the body. Two hundred and fifty million infants are affected by Vitamin A deficiency. Among women in developing countries, 40% have iron deficiency anemia, which increases maternal and infant mortality rates, chances of stillbirth, cases of low birth weight babies, premature delivery, and probability of fetal brain damage. One way to prevent Vitamin A deficiency is to educate the mother on the many benefits of breastfeeding. Breastmilk is a natural source of Vitamin A, and supplies the suckling infant with enough Vitamin A.
Infectious diseases
Babies born in low to middle income countries in sub-Saharan Africa and southern Asia are at the highest risk of neonatal death. Bacterial infections of the bloodstream, lungs, and the brain's covering (meningitis) are responsible for 25% of neonatal deaths. Newborns can acquire infections during birth from bacteria that are present in their mother's reproductive tract. The mother may not be aware of the infection, or she may have an untreated pelvic inflammatory disease or sexually transmitted disease. These bacteria can move up the vaginal canal into the amniotic sac surrounding the baby. Maternal blood-borne infection is another route of bacterial infection from mother to baby. Neonatal infection is also more likely with the premature rupture of the membranes (PROM) of the amniotic sac.
Seven out of ten childhood deaths are due to infectious diseases: acute respiratory infection, diarrhea, measles, and malaria. Acute respiratory infection such as pneumonia, bronchitis, and bronchiolitis account for 30% of childhood deaths; 95% of pneumonia cases occur in the developing world. Diarrhea is the second-largest cause of childhood mortality in the world, while malaria causes 11% of childhood deaths. Measles is the fifth-largest cause of childhood mortality. Folic acid for mothers is one way to combat iron deficiency. A few public health measures used to lower levels of iron deficiency anemia include iodize salt or drinking water, and include vitamin A and multivitamin supplements into a mother's diet. A deficiency of this vitamin causes certain types of anemia (low red blood cell count).
Environmental
Infant mortality rate can be a measure of a nation's health and social condition. It is a composite of a number of component rates which have their separate relationship with various social factors and can often be seen as an indicator to measure the level of socioeconomic disparity within a country.
Organic water pollution is a better indicator of infant mortality than health expenditures per capita. Water contaminated with various pathogens houses a host of parasitic and microbial infections. Infectious disease and parasites are carried via water pollution from animal wastes. Areas of low socioeconomic status are more prone to inadequate plumbing infrastructure, and poorly maintained facilities. The burning of inefficient fuels doubles the rate of children under 5 years old with acute respiratory tract infections. Climate and geography often play a role in sanitation conditions. For example, the inaccessibility of clean water exacerbates poor sanitation conditions.
People who live in areas where particulate matter (PM) air pollution is higher tend to have more health problems across the board. Short-term and long-term effects of ambient air pollution are associated with an increased mortality rate, including infant mortality. Air pollution is consistently associated with post neonatal mortality due to respiratory effects and sudden infant death syndrome. Specifically, air pollution is highly associated with SIDs in the United States during the post-neonatal stage. High infant mortality is exacerbated because newborns are a vulnerable subgroup that is affected by air pollution. Newborns who were born into these environments are no exception. Women who are exposed to greater air pollution on a daily basis who are pregnant should be closely watched by their doctors, as well as after the baby is born. Babies who live in areas with less air pollution have a greater chance of living until their first birthday. As expected, babies who live in environments with more air pollution are at greater risk for infant mortality. Areas that have higher air pollution also have a greater chance of having a higher population density, higher crime rates and lower income levels, all of which can lead to higher infant mortality rates.
The key pollutant for infant mortality rates is carbon monoxide. Carbon monoxide is a colorless, odorless gas that does great harm especially to infants because of their immature respiratory system. Another major pollutant is second-hand smoke, which is a pollutant that can have detrimental effects on a fetus. According to the American Journal of Public Health, "in 2006, more than 42 000 Americans died of second hand smoke-attributable diseases, including more than 41 000 adults and nearly 900 infants ... fully 36% of the infants who died of low birth weight caused by exposure to maternal smoking in utero were Blacks, as were 28% of those dying of respiratory distress syndrome, 25% dying of other respiratory conditions, and 24% dying of sudden infant death syndrome." The American Journal of Epidemiology also stated that "Compared with nonsmoking women having their first birth, women who smoked less than one pack of cigarettes per day had a 25% greater risk of mortality, and those who smoked one or more packs per day had a 56% greater risk. Among women having their second or higher birth, smokers experienced 30% greater mortality than nonsmokers."
Modern research in the United States on racial disparities in infant mortality suggests a link between the institutionalized racism that pervades the environment and high rates of African American infant mortality. In synthesis of this research, it has been observed that "African American infant mortality remains elevated due to the social arrangements that exist between groups and the lifelong experiences responding to the resultant power dynamics of these arrangements."
It is important to note that infant mortality rates do not decline among African Americans even if their socio-economic status does improve. Parker Dominguez at the University of Southern California has made some headway in determining the reasoning behind this, claiming black women are more prone to psychological stress than other women of different races in the United States. Stress is a lead factor in inducing labor in pregnant women, and therefore high levels of stress during pregnancy could lead to premature births that have the potential to be fatal for the infant.
Socio-economic factors
Social class is a major factor in infant mortality, both historically and today. Between 1912 and 1915, the Children's Bureau in the United States examined data across eight cities and nearly 23,000 live births. They discovered that lower incomes tend to correlate with higher infant mortality. In cases where the father had no income, the rate of infant mortality was 357% more than that for the highest income earners ($1,250+). Differences between races were also apparent. African-American mothers experience infant mortality at a rate 44% higher than average; however, research indicates that socio-economic factors do not totally account for the racial disparities in infant mortality.
While infant mortality is normally negatively correlated with GDP, there may indeed be some opposing short-term effects from a recession. A recent study by The Economist showed that economic slowdowns reduce the amount of air pollution, which results in a lower infant mortality rate. In the late 1970s and early 1980s, the recession's impact on air quality is estimated to have saved around 1,300 US babies. It is only during deep recessions that infant mortality increases. According to Norbert Schady and Marc-François Smitz, recessions when GDP per capita drops by 15% or more increase infant mortality.
Social class dictates which medical services are available to an individual. Disparities due to socioeconomic factors have been exacerbated by advances in medical technology. Developed countries, most notably the United States, have seen a divergence between those living in poverty who cannot afford medical advanced resources, leading to an increased chance of infant mortality, and others.
War
In policy, there is a lag time between realization of a problem's possible solution and actual implementation of policy solutions. Infant mortality rates correlate with war, political unrest, and government corruption.
In most cases, war-affected areas will experience a significant increase in infant mortality rates. Having a war taking place where a woman is planning on having a baby is not only stressful on the mother and fetus, but also has several detrimental effects.
However, many other significant factors influence infant mortality rates in war-torn areas. Health care systems in developing countries in the midst of war often collapse. Attaining basic medical supplies and care becomes increasingly difficult. During the Yugoslav Wars in the 1990s Bosnia experienced a 60% decrease in child immunizations. Preventable diseases can quickly become epidemic given the medical conditions during war.
Many developing countries rely on foreign aid for basic nutrition. Transport of aid becomes significantly more difficult in times of war. In most situations the average weight of a population will drop substantially. Expecting mothers are affected even more by lack of access to food and water. During the Yugoslav Wars in Bosnia the number of premature babies born increased and the average birth weight decreased.
There have been several instances in recent years of systematic rape as a weapon of war. Women who become pregnant as a result of war rape face even more significant challenges in bearing a healthy child. Studies suggest that women who experience sexual violence before or during pregnancy are more likely to experience infant death in their children. Causes of infant mortality in abused women range from physical side effects of the initial trauma to psychological effects that lead to poor adjustment to society. Many women who became pregnant by rape in Bosnia were isolated from their hometowns making life after childbirth exponentially more difficult.
Medicine and biology
Developing countries have a lack of access to affordable and professional health care resources, and skilled personnel during deliveries. Countries with histories of extreme poverty also have a pattern of epidemics, endemic infectious diseases, and low levels of access to maternal and child healthcare.
The American Academy of Pediatrics recommends that infants need multiple doses of vaccines such as diphtheria-tetanus-acellular pertussis vaccine, Haemophilus influenzae type b (Hib) vaccine, Hepatitis B (HepB) vaccine, inactivated polio vaccine (IPV), and pneumococcal vaccine (PCV). Research was conducted by the Institute of Medicine's Immunization Safety Review Committee concluded that there is no relationship between these vaccines and risk of SIDS in infants. This tells us that not only is it extremely necessary for every child to get these vaccines to prevent serious diseases, but there is no reason to believe that if your child does receive an immunization that it will have any effect on their risk of SIDS.
Economics
Political modernization perspective, the neo-classical economic theory that scarce goods are most effectively distributed to the market, say that the level of political democracy influences the rate of infant mortality. Developing nations with democratic governments tend to be more responsive to public opinion, social movements, and special interest groups for issues like infant mortality. In contrast, non-democratic governments are more interested in corporate issues and less so in health issues. Democratic status effects the dependency a nation has towards its economic state via export, investments from multinational corporations and international lending institutions.
Levels of socioeconomic development and global integration are inversely related to a nation's infant mortality rate. Dependency perspective occurs in a global capital system. A nation's internal impact is highly influenced by its position in the global economy and has adverse effects on the survival of children in developing countries. Countries can experience disproportionate effects from its trade and stratification within the global system. It aids in the global division of labor, distorting the domestic economy of developing nations. The dependency of developing nations can lead to a reduce rate of economic growth, increase income inequality inter- and intra-national, and adversely affects the wellbeing of a nation's population. A collective cooperation between economic countries plays a role in development policies in the poorer, peripheral, countries of the world.
These economic factors present challenges to governments' public health policies. If the nation's ability to raise its own revenues is compromised, governments will lose funding for its health service programs, including services that aim in decreasing infant mortality rates. Peripheral countries face higher levels of vulnerability to the possible negative effects of globalization and trade in relation to key countries in the global market.
Even with a strong economy and economic growth (measured by a country's gross national product), the advances of medical technologies may not be felt by everyone, lending itself to increasing social disparities.
Cultural
High rates of infant mortality occur in developing countries where financial and material resources are scarce and there is a high tolerance to high number of infant deaths. There are circumstances where a number of developing countries to breed a culture where situations of infant mortality such as favoring male babies over female babies are the norm. In developing countries such as Brazil, infant mortality rates are commonly not recorded due to failure to register for death certificates. Failure to register is mainly due to the potential loss of time and money and other indirect costs to the family. Even with resource opportunities such as the 1973 Public Registry Law 6015, which allowed free registration for low-income families, the requirements to qualify hold back individuals who are not contracted workers.
Another cultural reason for infant mortality, such as what is happening in Ghana, is that "besides the obvious, like rutted roads, there are prejudices against wives or newborns leaving the house." Because of this it is making it even more difficult for the women and newborns to get the treatment that is available to them and that is needed.
Cultural influences and lifestyle habits in the United States can account for some deaths in infants throughout the years. According to the Journal of the American Medical Association "the post neonatal mortality risk (28 to 364 days) was highest among continental Puerto Ricans" compared to babies of the non-Hispanic race. Examples of this include teenage pregnancy, obesity, diabetes and smoking. All are possible causes of premature births, which constitute the second highest cause of infant mortality. Ethnic differences experienced in the United States are accompanied by higher prevalence of behavioral risk factors and sociodemographic challenges that each ethnic group faces.
Gender favoritism
Historically, males have had higher infant mortality rates than females. The difference between male and female infant mortality rates have been dependent on environmental, social, and economic conditions. More specifically, males are biologically more vulnerable to infections and conditions associated with prematurity and development. Before 1970, the reasons for male infant mortality were due to infections, and chronic degenerative diseases. However, since 1970, certain cultures emphasizing males has led to a decrease in the infant mortality gap between males and females. Also, medical advances have resulted in a growing number of male infants surviving at higher rates than females due to the initial high infant mortality rate of males.
Genetic components results in newborn females being biologically advantaged when it comes to surviving their first birthday. Males, biologically, have lower chances of surviving infancy in comparison to female babies. As infant mortality rates saw a decrease on a global scale, the gender most affected by infant mortality changed from males experiences a biological disadvantage, to females facing a societal disadvantage. Some developing nations have social and cultural patterns that reflects adult discrimination to favor boys over girls for their future potential to contribute to the household production level. A country's ethnic composition, homogeneous versus heterogeneous, can explain social attitudes and practices. Heterogeneous level is a strong predictor in explaining infant mortality.
Birth spacing
Birth spacing is the time between births. Births spaced at least three years apart from one another are associated with the lowest rate of mortality. The longer the interval between births, the lower the risk for having any birthing complications, and infant, childhood and maternal mortality. Higher rates of pre-term births, and low birth weight are associated with birth to conception intervals of less than six months and abortion to pregnancy interval of less than six months. Shorter intervals between births increase the chances of chronic and general under-nutrition; 57% of women in 55 developing countries reported birth spaces shorter than three years; 26% report birth spacing of less than two years. Only 20% of post-partum women report wanting another birth within two years; however, only 40% are taking necessary steps such as family planning to achieve the birth intervals they want.
Unplanned pregnancies and birth intervals of less than twenty-four months are known to correlate with low birth weights and delivery complications. Also, women who are already small in stature tend to deliver smaller than average babies, perpetuating a cycle of being underweight.
Education
The mother's educational attainment and literacy are correlated with age of first pregnancy, and probability that the mother attain prenatal and postnatal care. Mothers with a secondary education have a higher probability of waiting until a later age to get pregnant. Once pregnant, they are also more likely to get prenatal and postnatal care, and deliver their child in the presence of a skilled attendant. Women who finish at least a primary-level education have improved nutrition, medical care, information access, and economic independence. Infants reap benefits such as healthy environments, improved nutrition, and medical care. Mothers with some level of education have a higher probability to breastfeeding. The duration of breastfeeding has the potential to influence the birth space. Women without any educational background tend to have children at an earlier age, thus their bodies are not yet mature enough to carry and deliver a child.
Prevention
Millennium Development Goals were created to improve the health and well being of people worldwide. Its fourth goal is to decrease the number of mortalities within the infant and childhood population by two thirds, a decrease from 95 to 31 deaths per 1000. Countries slow to abide by the Millennium Development Goal by 2015 are projected to have difficulty in reaching goal four.
Public health
Reductions in infant mortality are possible in any stage of a country's development. Rate reductions are evidence that a country is advancing in human knowledge, social institutions and physical capital. Governments can reduce the mortality rates by addressing the combined need for education (such as universal primary education), nutrition, and access to basic maternal and infant health services. A policy focus has the potential to aid those most at risk for infant and childhood mortality allows rural, poor and migrant populations.
Reducing chances of babies being born at low birth weights and contracting pneumonia can be accomplished by improving air quality. Improving hygiene can prevent infant mortality. Home-based technology to chlorinate, filter, and solar disinfection for organic water pollution could reduce cases of diarrhea in children by up to 48%. Improvements in food supplies and sanitation has been shown to work in the United States' most vulnerable populations, one being African Americans. Overall, women's health status need to remain high.
Simple behavioral changes, such as hand washing with soap, can significantly reduce the rate of infant mortality from respiratory and diarrheal diseases. According to UNICEF, hand washing with soap before eating and after using the toilet can save more lives of children than any single vaccine or medical intervention, by cutting deaths from diarrhea and acute respiratory infections.
Future problems for mothers and babies can be prevented. It is important that women of reproductive age adopt healthy behaviors in everyday life, such as taking folic acid, maintaining a healthy diet and weight, being physically active, avoiding tobacco use, and avoiding excessive alcohol and drug use. If women follow some of the above guidelines, later complications can be prevented to help decrease the infant mortality rates. Attending regular prenatal care check-ups will help improve the baby's chances of being delivered in safer conditions and surviving.
Focusing on preventing preterm and low birth weight deliveries throughout all populations can help to eliminate cases of infant mortality and decrease health care disparities within communities. In the United States, these two goals have decreased infant mortality rates on a regional population, it has yet to see further progress on a national level.
Medical treatments
Technological advances in medicine would decrease the infant mortality rate and an increased access to such technologies could decrease racial and ethnic disparities. It has been shown that technological determinants are influenced by social determinants. Those who cannot afford to utilize advances in medicine tend to show higher rates of infant mortality. Technological advances has, in a way, contributed to the social disparities observed today. Providing equal access has the potential to decrease socioeconomic disparities in infant mortality. Specifically, Cambodia is facing issues with a disease that is unfortunately killing infants. The symptoms only last 24 hours and the result is death. As stated if technological advances were increased in countries it would make it easier to find the solution to diseases such as this.
Cultural changes
Educated females practice a healthier lifestyle. The more educated a woman is the more likely she is to seek out care, give birth in the presence of a skilled attendant, breastfeed, and understand the consequences of HIV/AIDS. Improving women's health and social status is one way to ameliorate infant mortality. Status should rise for females seeking out education. Providing women access to family planning centers can educate mothers on how to plan ahead for their families. Educational means can also teach mothers on the beneficial health practices such as breastfeeding. Government recognizing birth space as a possible health intervention is now working towards making affordable contraception available.
Economic/Social policies
Granting women employment raises their status and autonomy. Having a gainful employment can raise the perceived worth of females. This can lead to an increase in the number of women getting an education and a decrease in the number of female infanticide. In the social modernization perspective, education leads to development. Higher number of skilled workers means more earning and further economic growth. According to the economic modernization perspective, this is one type economic growth viewed as the driving force behind the increase in development and standard of living in a country. This is further explained by the modernization theory- economic development promotes physical wellbeing. As economy rises, so do technological advances and thus, medical advances in access to clean water, health care facilities, education, and diet. These changes may decrease infant mortality.
Economically, governments could reduce infant mortality by building and strengthening capacity in human resources. Increasing human resources such as physicians, nurses, and other health professionals will increase the number of skilled attendants and the number of people able to give out immunized against diseases such as measles. Increasing the number of skilled professionals is negatively correlated with maternal, infant, and childhood mortality. Between 1960 and 2000, the infant mortality rate decreased by half as the number of physicians increased by four folds. With the addition of one physician to every 1000 persons in a population, infant mortality will reduce by 30%.
In certain parts of the U.S., specific modern programs aim to reduce levels of infant mortality. An example of one such program is the 'Healthy Me, Healthy You' program based in Northeast Texas. It intends to identify factors that contribute to negative birth outcomes throughout a 37-county area. An additional program that aims to reduce infant mortality is the "Best Babies Zone" (BBZ) based at the University of California, Berkeley. The BBZ uses the life course approach to address the structural causes of poor birth outcomes and toxic stress in three U.S. neighborhoods. By employing community-generated solutions, the Best Babies Zone's ultimate goal is to achieve health equity in communities that are disproportionately impacted by infant death.
Differences in measurement
The infant mortality rate correlates very strongly with, and is among the best predictors of, state failure. IMR is therefore also a useful indicator of a country's level of health or development, and is a component of the physical quality of life index.
However, the method of calculating IMR often varies widely between countries, and is based on how they define a live birth and how many premature infants are born in the country. Reporting of infant mortality rates can be inconsistent, and may be understated, depending on a nation's live birth criterion, vital registration system, and reporting practices. The reported IMR provides one statistic which reflects the standard of living in each nation. Changes in the infant mortality rate reflect social and technical capacities of a nation's population. The World Health Organization (WHO) defines a live birth as any infant born demonstrating independent signs of life, including breathing, heartbeat, umbilical cord pulsation or definite movement of voluntary muscles. This definition is used in Austria, for example. The WHO definition is also used in Germany, but with one slight modification: muscle movement is not considered to be a sign of life. Many countries, however, including certain European states (e.g. France) and Japan, only count as live births cases where an infant breathes at birth, which makes their reported IMR numbers somewhat lower and increases their rates of perinatal mortality. In the Czech Republic and Bulgaria, for instance, requirements for live birth are even higher.
Although many countries have vital registration systems and certain reporting practices, there are many inaccuracies, particularly in undeveloped nations, in the statistics of the number of infants dying. Studies have shown that comparing three information sources (official registries, household surveys, and popular reporters) that the "popular death reporters" are the most accurate. Popular death reporters include midwives, gravediggers, coffin builders, priests, and others—essentially people who knew the most about the child's death. In developing nations, access to vital registries, and other government-run systems which record births and deaths, is difficult for poor families for several reasons. These struggles force stress on families, and make them take drastic measures in unofficial death ceremonies for their deceased infants. As a result, government statistics will inaccurately reflect a nation's infant mortality rate. Popular death reporters have first-hand information, and provided this information can be collected and collated, can provide reliable data which provide a nation with accurate death counts and meaningful causes of deaths that can be measured/studied.
UNICEF uses a statistical methodology to account for reporting differences among countries:
UNICEF compiles infant mortality country estimates derived from all sources and methods of estimation obtained either from standard reports, direct estimation from micro data sets, or from UNICEF's yearly exercise. In order to sort out differences between estimates produced from different sources, with different methods, UNICEF developed, in coordination with WHO, the WB and UNSD, an estimation methodology that minimizes the errors embodied in each estimate and harmonize trends along time. Since the estimates are not necessarily the exact values used as input for the model, they are often not recognized as the official IMR estimates used at the country level. However, as mentioned before, these estimates minimize errors and maximize the consistency of trends along time.
Another challenge to comparability is the practice of counting frail or premature infants who die before the normal due date as miscarriages (spontaneous abortions) or those who die during or immediately after childbirth as stillborn. Therefore, the quality of a country's documentation of perinatal mortality can matter greatly to the accuracy of its infant mortality statistics. This point is reinforced by the demographer Ansley Coale, who finds dubiously high ratios of reported stillbirths to infant deaths in Hong Kong and Japan in the first 24 hours after birth, a pattern that is consistent with the high recorded sex ratios at birth in those countries. It suggests not only that many female infants who die in the first 24 hours are misreported as stillbirths rather than infant deaths, but also that those countries do not follow WHO recommendations for the reporting of live births and infant deaths.
Another seemingly paradoxical finding, is that when countries with poor medical services introduce new medical centers and services, instead of declining, the reported IMRs often increase for a time. This is mainly because improvement in access to medical care is often accompanied by improvement in the registration of births and deaths. Deaths that might have occurred in a remote or rural area, and not been reported to the government, might now be reported by the new medical personnel or facilities. Thus, even if the new health services reduce the actual IMR, the reported IMR may increase.
Collecting the accurate statistics of infant mortality rate could be an issue in some rural communities in developing countries. In those communities, some other alternative methods for calculating infant mortality rate are emerged, for example, popular death reporting and household survey. The country-to-country variation in child mortality rates is huge, and growing wider despite the progress. Among the world's roughly 200 nations, only Somalia showed no decrease in the under-5 mortality rate over the past two decades.The lowest rate in 2011 was in Singapore, which had 2.6 deaths of children under age 5 per 1,000 live births. The highest was in Sierra Leone, which had 185 child deaths per 1,000 births. The global rate is 51 deaths per 1,000 births. For the United States, the rate is eight per 1,000 births.
Infant mortality rate (IMR) is not only a group of statistic but instead it is a reflection of the socioeconomic development and effectively represents the presence of medical services in the countries. IMR is an effective resource for the health department to make decision on medical resources reallocation. IMR also formulates the global health strategies and help evaluate the program success. The existence of IMR helps solve the inadequacies of the other vital statistic systems for global health as most of the vital statistic systems usually neglect the infant mortality statistic number from the poor. There are certain amounts of unrecorded infant deaths in the rural area as they do not have information about infant mortality rate statistic or do not have the concept about reporting early infant death.
Europe and America
The exclusion of any high-risk infants from the denominator or numerator in reported IMRs can cause problems in making comparisons. Many countries, including the United States, Sweden and Germany, count an infant exhibiting any sign of life as alive, no matter the month of gestation or the size, but according to United States some other countries differ in these practices. All of the countries named adopted the WHO definitions in the late 1980s or early 1990s, which are used throughout the European Union. However, in 2009, the US CDC issued a report that stated that the American rates of infant mortality were affected by the United States' high rates of premature babies compared to European countries. It also outlined the differences in reporting requirements between the United States and Europe, noting that France, the Czech Republic, Ireland, the Netherlands, and Poland do not report all live births of babies under 500 g and/or 22 weeks of gestation. However, the differences in reporting are unlikely to be the primary explanation for the United States' relatively low international ranking. Rather, the report concluded that primary reason for the United States’ higher infant mortality rate when compared with Europe was the United States’ much higher percentage of preterm births. There are a number of factors which may account for this higher rate of preterm births, which include obesity or poor prenatal care.
The US National Institute of Child Health and Human Development (NICHD) has made great strides in lowering US infant mortality rates. Since the institute was created the US infant mortality rate has dropped 70%, in part due to their research.
Russia
Until the 1990s, Russia and the Soviet Union did not count, as a live birth or as an infant death, extremely premature infants (less than 1,000 g, less than 28 weeks gestational age, or less than 35 cm in length) that were born alive (breathed, had a heartbeat, or exhibited voluntary muscle movement) but failed to survive for at least seven days. Although such extremely premature infants typically accounted for only about 0.5% of all live-born children, their exclusion from both the numerator and the denominator in the reported IMR led to an estimated 22%–25% lower reported IMR. In some cases, too, perhaps because hospitals or regional health departments were held accountable for lowering the IMR in their catchment area, infant deaths that occurred in the 12th month were "transferred" statistically to the 13th month (i.e., the second year of life), and thus no longer classified as an infant death.
Brazil
In certain rural developing areas, such as northeastern Brazil, infant births are often not recorded in the first place, resulting in the discrepancies between the infant mortality rate (IMR) and the actual amount of infant deaths. Access to vital registry systems for infant births and deaths is an extremely difficult and expensive task for poor parents living in rural areas. Government and bureaucracies tend to show an insensitivity to these parents and their recent suffering from a lost child, and produce broad disclaimers in the IMR reports that the information has not been properly reported, resulting in these discrepancies. Little has been done to address the underlying structural problems of the vital registry systems in respect to the lack of reporting from parents in rural areas, and in turn has created a gap between the official and popular meanings of child death. It is also argued that the bureaucratic separation of vital death recording from cultural death rituals is to blame for the inaccuracy of the infant mortality rate (IMR). Vital death registries often fail to recognize the cultural implications and importance of infant deaths. It is not to be said that vital registry systems are not an accurate representation of a region's socio-economic situation, but this is only the case if these statistics are valid, which is unfortunately not always the circumstance. "Popular death reporters" is an alternative method for collecting and processing statistics on infant and child mortality. Many regions may benefit from "popular death reporters" who are culturally linked to infants may be able to provide more accurate statistics on the incidence of infant mortality. According to ethnographic data, "popular death reporters" refers to people who had inside knowledge of anjinhos, including the grave-digger, gatekeeper, midwife, popular healers etc. —— all key participants in mortuary rituals. By combining the methods of household surveys, vital registries, and asking "popular death reporters" this can increase the validity of child mortality rates, but there are many barriers that can reflect the validity of our statistics of infant mortality. One of these barriers are political economic decisions. Numbers are exaggerated when international funds are being doled out; and underestimated during reelection.
The bureaucratic separation of vital death reporting and cultural death rituals stems in part due to structural violence. Individuals living in rural areas of Brazil need to invest large capital for lodging and travel in order to report infant birth to a Brazilian Assistance League office. The negative financial aspects deters registration, as often individuals are of lower income and cannot afford such expenses. Similar to the lack of birth reporting, families in rural Brazil face difficult choices based on already existing structural arrangements when choosing to report infant mortality. Financial constraints such as reliance on food supplementations may also lead to skewed infant mortality data.
In developing countries such as Brazil the deaths of impoverished infants are regularly unrecorded into the countries vital registration system; this causes a skew statistically. Culturally validity and contextual soundness can be used to ground the meaning of mortality from a statistical standpoint. In northeast Brazil they have accomplished this standpoint while conducting an ethnographic study combined with an alternative method to survey infant mortality. These types of techniques can develop quality ethnographic data that will ultimately lead to a better portrayal of the magnitude of infant mortality in the region. Political economic reasons have been seen to skew the infant mortality data in the past when governor Ceara devised his presidency campaign on reducing the infant mortality rate during his term in office. By using this new way of surveying, these instances can be minimized and removed, overall creating accurate and sound data.
Global trends
For the world, and for both less developed countries (LDCs) and more developed countries (MDCs), IMR declined significantly between 1960 and 2001. According to the State of the World's Mothers report by Save the Children, the world IMR declined from 126 in 1960 to 57 in 2001.
However, IMR was, and remains, higher in LDCs. In 2001, the IMR for LDCs (91) was about 10 times as large as it was for MDCs (8). On average, for LDCs, the IMR is 17 times as higher than that of MDCs. Also, while both LDCs and MDCs made significant reductions in infant mortality rates, reductions among less developed countries are, on average, much less than those among the more developed countries.
A factor of about 67 separate countries with the highest and lowest reported infant mortality rates. The top and bottom five countries by this measure (taken from The World Factbook's 2012 estimates) are shown below.
According to Guillot, Gerland, Pelletier and Saabneh "birth histories, however, are subject to a number of errors, including omission of deaths and age misreporting errors."
In the United States
The infant mortality rate in the US decreased by 2.3% to a historic low of 582 infant deaths per 100,000 live births in 2014.
While the United States spends exponentially more on health care than any other country in the world, of the 27 developed countries, the U.S. has the highest IMR rate overall. While most of these other countries have more of a homogeneous population, the racial differences and divides within the United States prove to be more than simply differences. Based on race, there are chasms between the Infant Mortality Rate by race. It is not beneficial to assign one IMR to the entire country as the rate fluctuates drastically. Many theories have been explored as to why these racial differences exist with socio economic factors usually coming out as a reasonable explanation. However, more studies have been conducted around this matter, and the largest advancement is around the idea of stress and how it affects pregnancy.
In the 1850s, the infant mortality rate in the United States was estimated at 216.8 per 1,000 babies born for whites and 340.0 per 1,000 for African Americans, but rates have significantly declined in the West in modern times. This declining rate has been mainly due to modern improvements in basic health care, technology, and medical advances. In the last century, the infant mortality rate has decreased by 93%. Overall, the rates have decreased drastically from 20 deaths in 1970 to 6.9 deaths in 2003 (per every 1000 live births). In 2003, the leading causes of infant mortality in the United States were congenital anomalies, disorders related to immaturity, SIDS, and maternal complications. Babies born with low birth weight increased to 8.1% while cigarette smoking during pregnancy declined to 10.2%. This reflected the amount of low birth weights concluding that 12.4% of births from smokers were low birth weights compared with 7.7% of such births from non-smokers. According to the New York Times, "the main reason for the high rate is preterm delivery, and there was a 10% increase in such births from 2000 to 2006." Between 2007 and 2011, however, the preterm birth rate has decreased every year. In 2011 there was a 11.73% rate of babies born before the 37th week of gestation, down from a high of 12.80% in 2006.
Economic expenditures on labor and delivery and neonatal care are relatively high in the United States. A conventional birth averages 9,775 USD with a C-section costing 15,041 USD. Preterm births in the US have been estimated to cost $51,600 per child, with a total yearly cost of $26.2 billion. Despite this spending, several reports state that infant mortality rate in the United States is significantly higher than in other developed nations. Estimates vary; the CIA's World Factbook ranks the US 55th internationally in 2014, with a rate of 6.17, while the UN figures from 2005-2010 place the US 34th.
Aforementioned differences in measurement could play a substantial role in the disparity between the US and other nations. A non-viable live birth in the US could be registered as a stillbirth in similarly developed nations like Japan, Sweden, Norway, Ireland, the Netherlands, and France – thereby reducing the infant death count. Neonatal intensive care is also more likely to be applied in the US to marginally viable infants, although such interventions have been found to increase both costs and disability. A study following the implementation of the Born Alive Infant Protection Act of 2002 found universal resuscitation of infants born between 20–23 weeks increased the neonatal spending burden by $313.3 million while simultaneously decreasing quality-adjusted life years by 329.3.
The vast majority of research conducted in the late twentieth and early twenty-first century indicates that African-American infants are more than twice as likely to die in their first year of life than white infants. Although following a decline from 13.63 to 11.46 deaths per 1000 live births from 2005 to 2010, non-Hispanic black mothers continued to report a rate 2.2 times as high as that for non-Hispanic white mothers.
Contemporary research findings have demonstrated that nationwide racial disparities in infant mortality are linked to the experiential state of the mother and that these disparities cannot be totally accounted for by socio-economic, behavioral or genetic factors. The Hispanic paradox, an effect observed in other health indicators, appears in the infant mortality rate, as well. Hispanic mothers see an IMR comparable to non-Hispanic white mothers, despite lower educational attainment and economic status. A study in North Carolina, for example, concluded that "white women who did not complete high school have a lower infant mortality rate than black college graduates." According to Mustillo's CARDIA (Coronary Artery Risk Development in Young Adults) study, "self reported experiences of racial discrimination were associated with pre-term and low-birthweight deliveries, and such experiences may contribute to black-white disparities in prenatal outcomes." Likewise, dozens of population-based studies indicate that "the subjective, or perceived experience of racial discrimination is strongly associated with an increased risk of infant death and with poor health prospects for future generations of African Americans."
African American Infant Mortality in the United States
While earlier parts of this article have addressed the racial differences in infant deaths, a closer look into the affects of racial differences within the country is necessary to view discrepancies. Non-Hispanic Black women lead all other racial groups in IMR with a rate of 11.3, over double that of white women in the United States. While the popular argument leads to the idea that due to the trend of a lower socio-economic status had by black women there is in an increased likelihood of a child suffering. While this does correlate, the theory that it is the contributing factor falls apart when we look at Latino IMR in the United States. Latino people are almost just as likely to experience poverty as blacks in the U.S., however, the Infant Mortality Rate of Latinos is much closer to white women than it is to black women. The Poverty Rates of blacks and Latinos are 24.1% and 21.4% respectively. If there is a direct correlation, then the IMR of these two groups should be rather similar, however, blacks have an IMR double that of Latinos. Also, as black women move out of poverty or never experienced it in the first place, their IMR is not much lower than their counterparts experiencing higher levels of poverty.
Some believe black women are predisposed to a higher IMR, meaning ancestrally speaking, all black women from African descent should experience an elevated rate. This theory is quickly disproven by looking at women of African descent who have immigrated to the United States. These women who come from a completely different social context are not prone to the incredibly high IMR experienced by American-born black women.
Tyan Parker Dominguez at the University of Southern California offers a theory to explain the disproportionally high IMR among black women in the United States. She claims African American women experience stress at much higher rates than any other group in the country. Stress produces particular hormones that induce labor and contribute to other pregnancy problems. Considering early births are one of the leading causes of death of infants under the age of one, induced labor is a very legitimate factor. The idea of stress spans socio-economic status as Parker Dominguez claims stress for lower-class women comes from unstable family life and chronic worry over poverty. For black middle-class women, battling racism, real or perceived, can be an extreme stressor.
Arline Geronimus, a professor at the University of Michigan School of Public Health calls the phenomenon "weathering." She claims constantly dealing with disadvantages and racial prejudice causes black women's birth outcomes to deteriorate with age. Therefore, younger black women may experience stress with pregnancy due to social and economic factors, but older women experience stress at a compounding rate and therefore have pregnancy complications aside from economic factors.
Cigarette smoking has always been seen as a cause of low birth weights and fetal developmental issues, however, it is possible due to a study done by Newton and Hunt cigarettes, while incredibly harmful to the human body, may not be core reason for pregnancy issues. People generally smoke due to stress, and therefore stress could in fact be the other complications. This study was not entirely conclusive, but it did show that cigarette smoking had a strong effect on the stress of the fetus.
Strides have been made however to combat this epidemic. In Los Angeles County, health officials have partnered with non-profits around the city to help black women after the delivery of their child. One non-profit in particular has made a large impact on many lives is Great Beginnings For Black Babies in Inglewood. The non-profit centers around helping women deal with stress by forming support networks, keeping an open dialogue around race and family life, and also finding these women a secure place in the workforce.
History
The leading causes of infant mortality have changed over time. Unpasteurized milk was the leading cause of infant mortality late in the 19th century. Pasteurization of milk cut infant mortality by around 3/4.
Other meanings
In reliability engineering, "infant mortality" refers to the failures that occur in the first part of the bathtub curve.