
Specialty pulmonology ICD-9-CM 466.1 MedlinePlus 000975 | ICD-10 J21 DiseasesDB 1701 eMedicine emerg/365 | |
 | ||
Bronchiolitis is inflammation of the bronchioles, the smallest air passages of the lungs. It usually occurs in children less than two years of age with the majority being aged between three and six months. It presents with coughing, wheezing and shortness of breath which can cause some children difficulty in feeding. This inflammation is usually caused by respiratory syncytial virus (70% of cases) and is much more common in the winter months.
Contents
- Signs and symptoms
- Causes
- Diagnosis
- Prevention
- Management
- High flow therapy
- Bronchodilators
- Nebulized hypertonic saline
- Non effective
- Epidemiology
- References
Treatment is typically supportive with oxygen, monitoring, fluid and nutrition perhaps by gastric tube or intravenously. The use of nebulized hypertonic saline is controversial with some reviews finding benefits and others not. There is insufficient evidence to support treatment with antibiotics, surfactant, chest physiotherapy, bronchodilators or nebulized epinephrine. Bronchiolitis is common, with up to one third of children being affected in their first year of life.
Signs and symptoms
In a typical case, an infant under two years of age develops cough, wheeze, and shortness of breath over one or two days. Crackles or wheeze are typical findings on listening to the chest with a stethoscope. The infant may be breathless for several days. After the acute illness, it is common for the airways to remain sensitive for several weeks, leading to recurrent cough and wheeze.
Some signs of severe disease include:
Causes
The term usually refers to acute viral bronchiolitis, a common disease in infancy. This is most commonly caused by respiratory syncytial virus (RSV, also known as human pneumovirus). Other viruses which may cause this illness include metapneumovirus, influenza, parainfluenza, coronavirus, adenovirus, and rhinovirus.
Studies have shown there is a link between voluntary caesarean birth and an increased prevalence of bronchiolitis. A recent study by Perth's Telethon Institute for Child Health Research has shown an 11% increase in hospital admissions for children delivered this way. Children born prematurely (less than 35 weeks), with a low birth weight or who have from congenital heart disease may have higher rates of bronchiolitis and are more likely to require hospital admission. There is evidence that breastfeeding provides some protection against bronchiolitis.
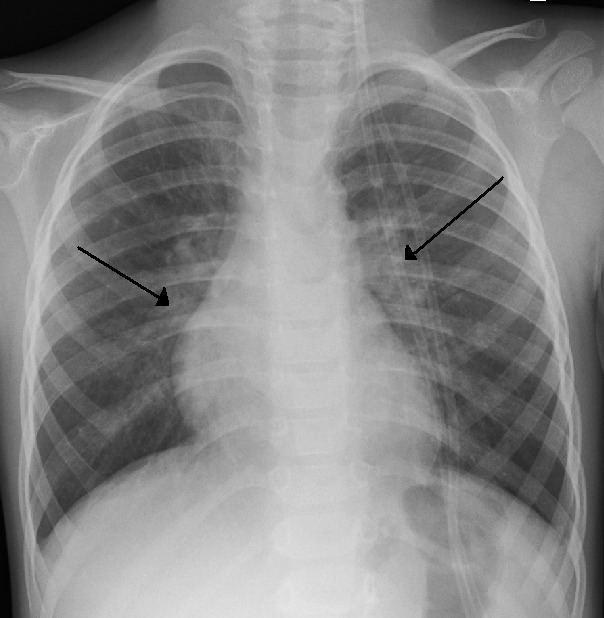
Diagnosis
The diagnosis is typically made by clinical examination. Chest X-ray is sometimes useful to exclude bacterial pneumonia, but not indicated in routine cases.
Testing for the specific viral cause can be done but has little effect on management and thus is not routinely recommended. RSV testing by direct immunofluorescence testing on nasopharyngeal aspirate had a sensitivity of 61% and specificity of 89%. Identification of those who are RSV-positive can help for: disease surveillance, grouping ("cohorting") people together in hospital wards to prevent cross infection, predicting whether the disease course has peaked yet, reducing the need for other diagnostic procedures (by providing confidence that a cause has been identified).
Infants with bronchiolitis between the age of two and three months have a second infection by bacteria (usually a urinary tract infection) less than 6% of the time. Preliminary studies have suggested that elevated procalcitonin levels may assist clinicians in determining the presence of bacterial coinfection, which could prevent unnecessary antibiotic use and costs.
Prevention
Prevention of bronchiolitis relies strongly on measures to reduce the spread of the viruses that cause respiratory infections (that is, handwashing, and avoiding exposure to those symptomatic with respiratory infections). In addition to good hygiene an improved immune system is a great tool for prevention. One way to improve the immune system is to feed the infant with breast milk, especially during the first month of life. Immunizations are available for premature infants who meet certain criteria (some cardiac and respiratory disorders) such as Palivizumab (a monoclonal antibody against RSV). Passive immunization therapy requires monthly injections during winter.
Management
Treatment of bronchiolitis is usually focused on the symptoms instead of the infection itself since the infection will run its course and complications are typically from the symptoms themselves. Without active treatment half of cases will go away in 13 days and 90% in three weeks.
High-flow therapy
High flow therapy with a high flow device that can provide precise flow/FiO2 and medical grade vapor is an important part of the management of bronchiolitis.
Bronchodilators
Although inhaled epinephrine has been shown to decrease initial hospital admissions and overall length of stay compared to placebo in some studies, meta-analyses have found that it has no effect on the rate of one week post-emergency department visits or length of stay (although it does lead to shorter stay versus salbutamol). Nebulized and inhaled salbutamol (sold in the USA as Ventolin HFA) has been shown to decrease initial hospital admission rates in some studies, but no clear effect on length of stay in meta-analysis. The Society of Hospital Medicine recommends against routine use of these or other bronchodilators in children with bronchiolitis: "Published guidelines do not advocate the routine use of bronchodilators in patients with bronchiolitis. Comprehensive reviews of the literature have demonstrated that the use of bronchodilators in children admitted to the hospital with bronchiolitis has no effect on any important outcomes. There is limited demonstration of clear impact of bronchodilator therapy upon the course of disease. Additionally, providers should consider the potential impact of adverse events upon the patient."
Nebulized hypertonic saline
Nebulized hypertonic saline (3%) is controversial with some reviews finding benefit and others not.
Non-effective
Currently other medications do not yet have evidence to support their use. Ribavirin is an antiviral drug which does not appear to be effective for bronchiolitis. Antibiotics are often given in case of a bacterial infection complicating bronchiolitis, but have no effect on the underlying viral infection. Corticosteroids have no proven benefit in bronchiolitis treatment and are not advised. DNAse has not been found to be effective.
Epidemiology
Bronchiolitis typically affects infants and children younger than two years, principally during the fall and winter . Bronchiolitis hospitalization has a peak incidence between two and six months of age and remains a significant cause of respiratory disease during the first two years of life. It is a leading cause of hospitalization in infants and young children.