
Specialty infectious disease ICD-9-CM 053.20 MedlinePlus 000858 | ICD-10 B02 DiseasesDB 29119 | |
 | ||
eMedicine med/1007 derm/180 emerg/823 oph/257 ped/996 | ||
Herpes zoster ophthalmicus (HZO) and also known as ophthalmic zoster is a disease characterised by reactivation of dormant varicella zoster virus residing within the ophthalmic nerve (the first division of the trigeminal nerve). This condition is an important subtype of shingles, representing 15% of all cases. Herpes zoster ophthalmicus is transmitted via direct contact or droplets. Varicella zoster virus is a DNA virus which produces acidophilic intranuclear inclusion bodies. The virus is neurotrophic in nature.
Contents
The frontal nerve is more commonly affected than the nasociliary nerve or lacrimal nerve.
Signs and symptoms
Any potential ocular involvement should be assessed by an ophthalmologist as complications such as episcleritis and uveitis may occur.
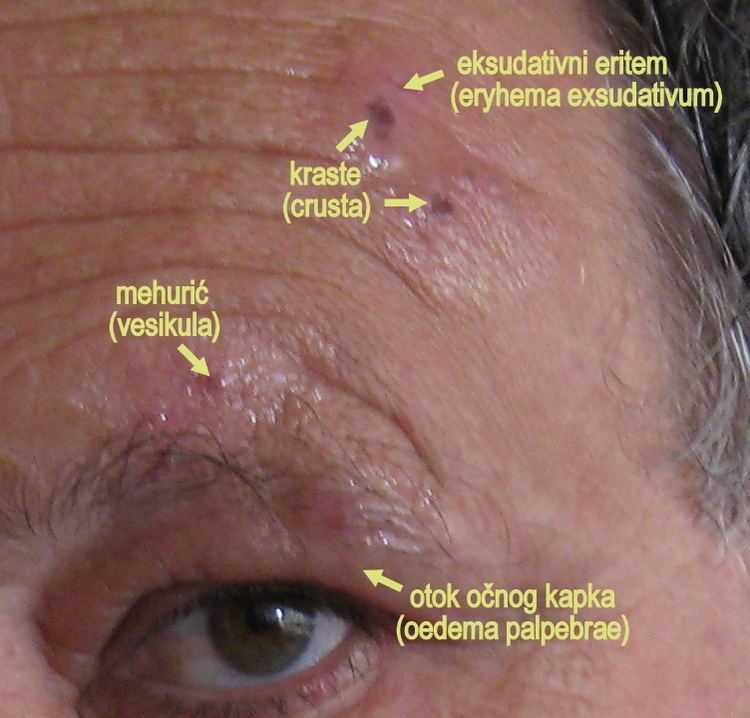
Skin
Cornea
Uveal
Anterior uveitis develops in 40–50% of cases with HZO within 2 weeks of onset of the skin rashes. Typical HZO keratitis at least mild iritis, especially if Hutchinson's sign is positive for the presence of vescicles upon the tip of the nose.
Features:
This non-granulomatous iridocyclitis is associated with:
HZO uveitis is associated with complications such as iris atrophy and secondary glaucoma are not uncommon. Complicated cataract may develop in the late stages of the disease.
Treatment
Treatment is usually with antivirals such as aciclovir orally.