
ICD-9-CM 642.6 MedlinePlus 000899 | ICD-10 O15 DiseasesDB 4068 eMedicine med/1905 emerg/796 | |
 | ||
Eclampsia is the onset of seizures (convulsions) in a woman with pre-eclampsia. Pre-eclampsia is a disorder of pregnancy in which there is high blood pressure and either large amounts of protein in the urine or other organ dysfunction. Onset may be before, during, or after delivery. Most often it is during the second half of pregnancy. The seizures are of the tonic–clonic type and typically last about a minute. Following the seizure there is typically either a period of confusion or coma. Complications include aspiration pneumonia, cerebral hemorrhage, kidney failure, and cardiac arrest. Pre-eclampsia and eclampsia are part of a larger group of conditions known as hypertensive disorders of pregnancy.
Contents
- Signs and symptoms
- Risk factors
- Mechanism
- Differential diagnosis
- Prevention
- Treatment
- Convulsions
- Blood pressure management
- Delivery
- Monitoring
- Etymology
- Popular culture
- References
Recommendations for prevention include aspirin in those at high risk, calcium supplementation in areas with low intake, and treatment of prior hypertension with medications. Exercise during pregnancy may also be useful. The use of intravenous or intramuscular magnesium sulfate improves outcomes in those with eclampsia and is generally safe. This is true in both the developed and developing world. Breathing may need to be supported. Other treatments may include blood pressure medications such as hydralazine and emergency delivery of the baby either vaginally or by cesarean section.
Pre-eclampsia is estimated to affect about 5% of deliveries while eclampsia affects about 1.4% of deliveries. In the developed world rates are about 1 in 2,000 deliveries due to improved medical care. Hypertensive disorders of pregnancy are one of the most common causes of death in pregnancy. They resulted in 29,000 deaths in 2013 – down from 37,000 deaths in 1990. Around one percent of women with eclampsia die. The word eclampsia is from the Greek term for lightning. The first known description of the condition was by Hippocrates in the 5th century BCE.
Signs and symptoms
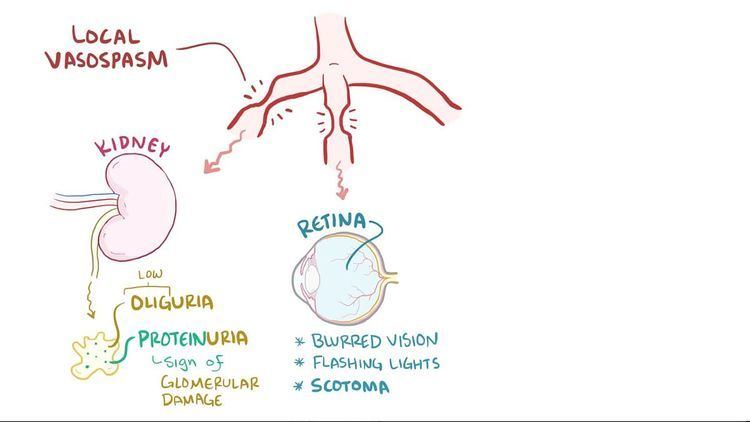
Typically the pregnant woman develops hypertension and proteinuria before the onset of a convulsion, the hallmark of eclampsia. Eclampsia is pre-eclampsia and seizures. Other cerebral signs may immediately precede the convulsion, such as nausea, vomiting, headaches, and cortical blindness. If the complication of multi-organ failure ensues, signs and symptoms of those failing organs will appear, such as abdominal pain, jaundice, shortness of breath, and diminished urine output.
The fetus may develop intrauterine growth retardation, and with maternal convulsions, bradycardia, and fetal distress. Placental bleeding, and placental abruption may also occur.
Sometimes the pregnant woman becomes comatose without preceding convulsions. Upon awakening from the coma, some experience amaurosis fugax: a "dark" and "fleeting" unilateral temporary blindness.
Risk factors
Eclampsia, like pre-eclampsia, tends to occur more commonly in first pregnancies and young mothers where it is thought that novel exposure to paternal antigens is involved. Furthermore, women with pre-existing vascular diseases (hypertension, diabetes, and nephropathy) or thrombophilic diseases such as the antiphospholipid syndrome are at higher risk to develop pre-eclampsia and eclampsia. Having a large placenta (multiple gestation, hydatidiform mole) also predisposes women to eclampsia. In addition, there is a genetic component: a woman whose mother or sister had the condition is at higher risk than otherwise. Women who have experienced eclampsia are at increased risk for pre-eclampsia/eclampsia in a later pregnancy. Pulmonary edema is a rather common complication of severe eclampsia affecting approximately 3% of the people with eclampsia: most is caused by too much intravenous fluid.
Mechanism
The presence of a placenta is required, and eclampsia resolves if it is removed. Reduced blood flow to the placenta (placental hypoperfusion) is a key feature of the process. It is accompanied by increased sensitivity of the maternal vasculature to agents which cause constriction of the small arteries, leading to reduced blood flow to multiple organs. Also, an activation of the coagulation cascade may lead to microthrombi formation, which can further impair blood flow. Thirdly, increased vascular permeability results in the shift of extracellular fluid from the blood to the interstitial space, with further reduction in blood flow, and edema. These events lead to hypertension; renal, pulmonary, and hepatic dysfunction; and cerebral edema with cerebral dysfunction and convulsions. Before symptoms appear, increased platelet and endothelial activation may be detected.
Placental hypoperfusion is linked to abnormal modelling of the fetal–maternal placental interface that may be immunologically mediated. The invasion of the trophoblast appears to be incomplete. The placenta produces the potent vasodilator adrenomedullin: it is reduced in pre-eclampsia and eclampsia. Other vasodilators are also reduced, including prostacyclin, thromboxane A2, nitric oxide, and endothelins, also leading to vasoconstriction. Many studies have suggested the importance of a woman's reduced immunological tolerance to her baby's father, whose genes are present in the young fetus and the placenta.
Eclampsia is a form of hypertensive encephalopathy: cerebral vascular resistance is reduced, leading to increased blood flow to the brain, cerebral edema and resultant convulsions. An eclamptic convulsion usually does not cause chronic brain damage unless intracranial haemorrhage occurs.
Differential diagnosis
Convulsions during pregnancy that are unrelated to pre-eclampsia need to be distinguished from eclampsia. Such disorders include seizure disorders as well as brain tumor, aneurysm of the brain, and medication- or drug-related seizures. Usually the presence of the signs of severe pre-eclampsia precede and accompany eclampsia, facilitating the diagnosis.
Investigations include: CBC, renal function test (RFT), liver function tests (LFT), coagulation screen, 24-hour urine creatinine and protein, and fetal/placental ultrasound.
Prevention
Detection and management of pre-eclampsia is critical to reduce the risk of eclampsia. Appropriate management of women with pre-eclampsia generally involves the use of magnesium sulphate to prevent convulsions.
Treatment
The four goals of the treatment of eclampsia are to stop and prevent further convulsions, to control the elevated blood pressure, to deliver the baby as promptly as possible, and to monitor closely for the onset of multi-organ failure.
Convulsions
Convulsions are prevented and treated using magnesium sulfate. The study demonstrating the effectiveness of magnesium sulfate for the management of eclampsia was first published in 1955. Serum magnesium concentrations associated with maternal toxicity as well as neonatal depression, hypotonia, and low Apgar scores are:
With intravenous administration the onset of anticonvulsant action is fast and lasts about 30 minutes. Following intramuscular administration the onset of action is about one hour and lasts for three to four hours. Effective anticonvulsant serum levels range from 2.5 to 7.5 mEq/liter. Magnesium is excreted solely by the kidneys at a rate proportional to the plasma concentration and glomerular filtration.
Even with therapeutic serum magnesium concentrations, recurrent convulsions may occur, and additional magnesium may be needed, but with close monitoring for respiratory, cardiac, and neurological depression. If magnesium administration with resultant high serum concentrations fail to control convulsions, the addition of other intravenous anticonvulsants may be used, facilitate intubation and mechanical ventilation, and to avoid magnesium toxicity including maternal thoracic muscle paralysis.
Magnesium sulfate results in better outcomes than diazepam, phenytoin or a combination of chlorpromazine, promethazine and pethidine.
Blood pressure management
The agents of choice for blood pressure control during eclampsia are hydralazine and/or labetalol. This is because of their effectiveness, lack of negative effects on the fetus, and mechanism of action.
Delivery
If the baby has not yet been delivered, steps need to be taken to stabilize the woman and deliver her speedily. This needs to be done even if the baby is immature, as the eclamptic condition is unsafe for both baby and mother. As eclampsia is a manifestation of a multiorgan failure, other organs (liver, kidney, lungs, cardiovascular system, and coagulation system) need to be assessed in preparation for a delivery (often a caesarean section), unless the woman is already in advanced labor. Regional anesthesia for caesarean section is contraindicated when a coagulopathy has developed.
Monitoring
Invasive haemodynamic monitoring may be elected in an eclamptic woman at risk for or with cardiac disease, renal disease, refractory hypertension, pulmonary edema, or poor urine output.
Etymology
The Greek noun "ἐκλαμψία", eklampsía, denotes a "light burst"; metaphorically, in this context, "sudden occurrence." The New Latin term first appeared in Johannes Varandaeus’ 1620 treatise on gynaecology Tractatus de affectibus Renum et Vesicae. The term toxemia of pregnancy is no longer recommended: placental toxins are not the cause of eclampsia occurrences, as previously believed.
Popular culture
In Downton Abbey, an historical drama television series, the character (in season 3, episode 5) Lady Sybil dies of eclampsia shortly after child birth.
In Call the Midwife, a medical drama television series set in London in the 1950s and 1960s, the character (in season 1, episode 4) named Margaret Jones is struck with pre-eclampsia, ultimately proceeding from a comatose condition to death. The term "toxemia" was also used for the condition, in the dialogue.