
Pronunciation /ləˈbɛtəlɔːl/ AHFS/Drugs.com Monograph Routes ofadministration oral, iv Protein binding 50% Molar mass 328.406 g/mol | Trade names Normodyne, Trandate MedlinePlus a685034 CAS ID 36894-69-6 Bioavailability 25% | |
 | ||
Pregnancycategory COne of few drugs used for PIH | ||
Labetalol
Labetalol, sold under the trade names Normodyne among others, is a mixed alpha/beta adrenergic antagonist that is used to treat high blood pressure. It can be given intravenously in severe hypertensive situations, or by mouth for long term hypertension management. Its dose and use is limited by its main side effect—postural hypotension, where there is a substantial drop in blood pressure when standing up.
Contents
- Labetalol
- Medical uses
- Special populations
- Common
- Rare
- Contraindications
- Chemistry
- Mechanism of Action
- Physiological Action
- Pharmacokinetics
- History
- References
Labetalol's dual alpha- and beta- blockade has different physiological effects in short- and long-term situations. In short-term, acute situations, labetalol decreases blood pressure by decreasing systemic vascular resistance with little effect on stroke volume, heart rate and cardiac output. During long-term use, labetalol can reduce heart rate during exercise while maintaining cardiac output by an increase in stroke volume.
Medical uses
Labetalol is effective in the management of hypertensive emergencies, postoperative hypertension, pheochromocytoma-associated hypertension, and rebound hypertension from beta blocker withdrawal.
It has a particular indication in the treatment of pregnancy-induced hypertension which is commonly associated with pre-eclampsia.
It is also used as an alternative in the treatment of severe hypertension.
Special populations
Pregnancy: Studies in lab animals showed no harm to the fetus. However, a comparable well-controlled study has not been performed in pregnant women.
Nursing: Breast milk has been shown to contain small amounts of labetalol (0.004% original dose). Prescribers should be cautious in the use of labetalol for nursing mothers.
Pediatric: No studies have established safety or usefulness in this population.
Geriatric: The elderly are more likely to experience dizziness when taking labetalol. Labetalol should be dosed with caution in the elderly and counseled on this side effect.
Common
Low blood pressure with standing is more severe and more common with IV formulation (58% vs 1%) and is often the reason larger doses of the oral formulation cannot be used.
Rare
Contraindications
Labetalol is contraindicated in people with overt cardiac failure, greater-than-first-degree heart block, severe bradycardia, cardiogenic shock, severe hypotension, anyone with a history of obstructive airway disease including asthma, and those with hypersensitivity to the drug.
Chemistry
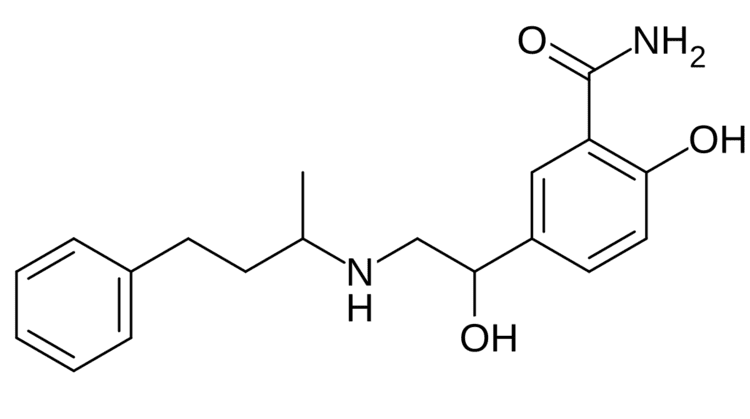
The minimum requirement for adrenergic agents is a primary or secondary amine separated from a substituted benzene ring by one or two carbons. This configuration results in strong agonist activity. As the size of the substituent attached to the amine becomes greater, particularly with respect to a t-butyl group, then the molecule typically is found to have receptor affinity without intrinsic activity, and is, therefore, an antagonist. Labetalol, with its 1-methyl-3-phenylpropyl substituted amine, is greater in size relative to a t-butyl group and therefore acts predominantly as an antagonist. The overall structure of labetalol is very polar. This was created by substituting the isopropyl group in the standard beta-blocker structure with an aralkyl group, including a carboxamide group on the meta position, and by adding a hydroxyl group on the para position.
Labetalol has two chiral carbons and consequently exists as four stereoisomers. Two of these isomers, the (S,S)- and (R,S)- forms are inactive. The third, the (S,R)-isomer, is a powerful α1 blocker. The fourth isomer, the (R,R)-isomer which is also known as dilevalol, is a mixed nonselective β blocker and selective α1 blocker. Labetalol is typically given as a racemic mixture to achieve both alpha and beta receptor blocking activity.
Labetalol acts by blocking alpha and beta adrenergic receptors, resulting in decreased peripheral vascular resistance without significant alteration of heart rate or cardiac output.
The β:α antagonism of labetalol is approximately 3:1.
It is chemically designated in International Union of Pure and Applied Chemistry (IUPAC) nomenclature as 2-hydroxy-5-[1-hydroxy-2-[(1-methyl-3-phenylpropyl)amino]ethyl]benzamide monohydrochloride.
Mechanism of Action
Labetalol is a dual alpha (α1) and beta (β1/β2) adrenergic receptor blocker and competes with other Catecholamines for binding to these sites. Its action on these receptors are potent and reversible. Labetalol is highly selective for postsynaptic alpha1- adrenergic, and non-selective for beta-adrenergic receptors. It is about equipotent in blocking both beta1- and beta2- receptors.
The amount of alpha to beta blockade depends on whether labetalol is administered orally or intravenously (IV). Orally, the ratio of alpha to β blockade is 1:3. Intravenously, alpha to β blockade ratio is 1:7. Thus, the labetalol can be thought to be a beta-blocker with some alpha-blocking effects. By comparison, labetalol is a weaker β-blocker than propranolol, and has a weaker affinity for alpha-receptors compared to Phentolamine.
Labetalol possesses intrinsic sympathomimetic activity. In particular, it is a partial agonist at beta2- receptors located in the vascular smooth muscle. Labetalol relaxes vascular smooth muscle by a combination of this partial beta2- agonism and through alpha1- blockade. Overall, this vasodilatory effect can decrease blood pressure.
Similar to local anesthetics and sodium channel blocking antiarrhythmics, labetalol also has membrane stabilizing activity. By decreasing sodium entry, labetalol decreases action potential firing and thus has local anesthetic activity.
Physiological Action
The physiological effects of labetalol when administered acutely (intravenously) are not predictable solely by their receptor blocking effect, i.e. blocking beta1- receptors should decrease heart rate, but labetalol does not. When labetalol is given in acute situations, it decreases the peripheral vascular resistance and systemic blood pressure while having little effect on the heart rate, cardiac output and stroke volume, despite its alpha1-, beta1- and beta2- blocking mechanism. These effects are mainly seen when the person is in the upright position.
Long term labetalol use also has different effects from other beta-blocking drugs. Other beta-blockers, such as propranolol, persistently reduce cardiac output during exercise. The peripheral vascular resistance decreases when labetalol is first administered. Continuous labetalol use further decreases peripheral vascular resistance. However, during exercise, cardiac output remains the same due to a compensatory mechanism that increases stroke volume. Thus, labetalol is able to reduce heart rate during exercise while maintaining cardiac output by the increase in stroke volume.
Pharmacokinetics
Labetalol, in animal models, was found to cross the blood-brain-barrier in only negligible amounts.
History
Labetalol was the first drug created that combined both alpha- and beta- adrenergic receptor blocking properties. It was created to potentially fix the compensatory reflex issue that occurred when blocking a single receptor subtype, i.e. vasoconstriction after blocking beta-receptors or tachycardia after blocking alpha receptors. Because the reflex from blocking the single receptor subtypes acted to prevent the lowering of blood pressure, it was postulated that weak blocking of both alpha- and beta- receptors could work together to decrease blood pressure.