
ICD-10 D48.5 (ILDS D48.540) ICD-O M8727/0 MeSH D004416 | ICD-9-CM 238.2 OMIM 155600 | |
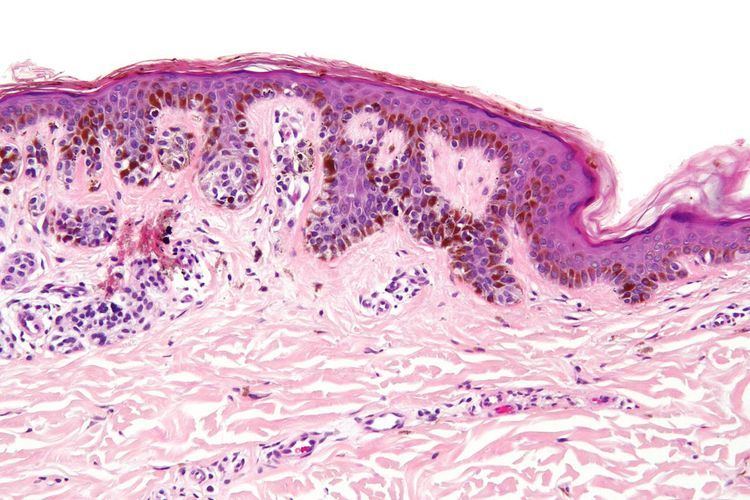 | ||
A dysplastic nevus or atypical mole is a nevus (mole) whose appearance is different from that of common moles. In 1992, the NIH recommended that the term "dysplastic nevus" be avoided in favor of the term "atypical mole". An atypical mole may also be referred to as an atypical melanocytic nevus, atypical nevus, B-K mole, Clark's nevus, dysplastic melanocytic nevus, or nevus with architectural disorder.
Contents
Dysplastic nevi often grow to larger than ordinary moles, and may have irregular and indistinct borders. Their color may not be uniform, and may range from light pink to very dark brown. They usually begin flat, but parts may raise above the skin surface. See ABCDE and "ugly duckling" characteristics below.
Dysplastic nevi can be found anywhere, but are most common on the trunk in men, and on the calves in women.
Cancer
According to the National Cancer Institute, researchers have shown that atypical moles are more likely than ordinary moles to develop into a type of skin cancer called melanoma. It is worth noting that the vast majority of atypical moles will never become malignant. However, numerous studies indicate that about half of melanomas arise from atypical moles. Evidence supporting this connection arises from clinical photodocumentation of evolving lesions, patient self-reports of changing lesions, pathology studies showing dysplastic nevi in histologic contiguity with melanoma, and epidemiology studies indicating that about half of individuals affected by melanoma also have atypical moles. Epidemiology studies have also shown that individuals with multiple dysplastic nevi are at much higher risk for developing melanomas. Because of this, moles should be checked regularly by a doctor or nurse specialist, especially if they look complex; grow larger; change in color or shape; or if any changes occur, such as itching, flaking or oozing.
Precaution for individuals with dysplastic nevi
Although there are limited data to support its efficacy, skin self-examination is frequently recommended for preventing melanoma (by identifying atypical moles that can be removed) or for early detection of existing tumors. Examination by a dermatologist has been shown to be beneficial for early melanoma detection. Some dermatologists recommend that an individual with either histologic diagnosis of dysplastic nevus, or clinically apparent atypical moles should be examined by an experienced dermatologist with dermatoscopy once a year (or more frequently).
The abbreviation ABCDE has been useful for helping health care providers and laypersons remember the key characteristics of a melanoma (see "ABCDE" mnemonic below). Changes (in shape, size, color, itching or bleeding) should be brought to the attention of a dermatologist .
A popular method for remembering the signs and symptoms of melanoma is the mnemonic "ABCDE":
The E is sometimes omitted, as in the ABCD guideline. A weakness in this system is the D. Many melanomas present themselves as lesions smaller than 6 mm in diameter. An astute physician will examine all abnormal moles, including ones less than 6 mm in diameter. Unfortunately for the average person, many seborrheic keratoses, some lentigo senilis, and even warts may have ABCD characteristics, and cannot be distinguished from a melanoma without a trained eye or dermatoscopy.
A recent and novel method of melanoma detection is the "Ugly Duckling Sign". It is simple, easy to teach, and highly effective in detecting melanoma. Simply, correlation of common characteristics of a person's skin lesion is made. Lesions which greatly deviate from the common characteristics are labeled as an "Ugly Duckling", and a dermatologist exam is required. The "Little Red Riding Hood" sign suggests that individuals with fair skin and light colored hair might prove more challenging. These fair-skinned individuals often have lightly pigmented or amelanotic melanomas which will not present with easy to observe color changes and variation in colors. The borders of these amelanotic melanomas are often indistinct, making visual identification without a dermatoscope (dermatoscopy) very difficult. A dermatoscope must be used to detect "ugly ducklings" among those with light skin or blonde/red hair.
People with a personal or family history of skin cancer or of dysplastic nevus syndrome (multiple atypical moles) should see a dermatologist at least once a year to be sure they are not developing melanoma.
Biopsy
When an atypical mole has been identified, a skin biopsy takes place in order to best diagnose it. Local anesthetic is used to numb the area, then the mole is biopsied. The biopsy material is then sent to a laboratory to be evaluated by a pathologist. A skin biopsy can be a punch, shave, or complete excision. The complete excision is the preferred method, but a punch biopsy can suffice if the patient has cosmetic concerns (i.e. the patient does not want a scar) and the lesion is small. A scoop or deep shave biopsy is often advocated, but should be avoided due to risk of a recurrent nevus, which can complicate future diagnosis of a melanoma, and the possibility that resulting scar tissue can obscure tumor depth if a melanoma is found to be present and re-excised.
Most dermatologists and dermatopathologists use a system devised by the NIH for classifying melanocytic lesions. In this classification, a nevus can be defined as benign, having atypia, or being a melanoma. A benign nevus is read as (or understood as) having no cytologic or architectural atypia. An atypical mole is read as having architectural atypia, and having (mild, moderate, or severe) cytologic (melanocytic) atypia. Usually, cytologic atypia is of more important clinical concern than architectural atypia. Usually, moderate to severe cytologic atypia will require further excision to make sure that the surgical margin is completely clear of the lesion.
The most important aspect of the biopsy report is that the pathologist indicates if the margin is clear (negative or free of melanocytic nevus), or if further tissue (a second surgery) is required. If this is not mentioned, usually a dermatologist or clinician will require further surgery if moderate to severe cytologic atypia is present – and if residual nevus is present at the surgical margin.
Dysplastic nevus syndrome
"Dysplastic nevus syndrome" refers to individuals who have high numbers of benign moles and also have dysplastic nevi. A small percent of these individuals are members of melanoma kindreds. Inherited dysplastic nevus syndrome is an autosomal dominant hereditary condition. Dysplastic nevi are more likely to undergo malignant transformation when they occur among members of melanoma families. At least one study indicates a cumulative lifetime risk of nearly 100% in individuals who have dysplastic nevi and are members of melanoma kindreds. Roughly half of melanomas arise "de novo" on clear skin growth, whereas the other half arise within atypical moles. Those with dysplastic nevi have an elevated risk of melanoma. Such persons need to be checked regularly for any changes in their moles and to note any new ones. In 40-50% of cases, the disorder has been linked with germline mutations in the CDKN2A gene, which codes for p16 (a regulator of cell division).