
Group Group II (ssDNA) Subfamily Parvovirinae Scientific name Canine parvovirus 2 Rank Species | Higher classification Protoparvovirus | |
 | ||
Similar Parvovirus, Feline distemper, Bordetella, Heartworm, Parvoviridae | ||
Canine parvovirus
Canine parvovirus type 2 (CPV2, colloquially parvo) is a contagious virus mainly affecting dogs, and thought to originate in cats. The current consensus is that the feline panleukopenia mutated into CPV2. Parvo is highly contagious and is spread from dog to dog by direct or indirect contact with their feces. Vaccines can prevent this infection, but mortality can reach 91% in untreated cases. Treatment often involves veterinary hospitalization. Canine parvovirus may infect other mammals; however, it will not infect humans.
Contents
- Canine parvovirus
- Signs
- Diagnosis
- Treatment
- Unconventional treatments
- History
- Pathophysiology
- Intestinal form
- Cardiac form
- Infection of the fetus
- Virology
- Variants
- Prevention and decontamination
- References
Signs
Dogs that develop the disease show signs of the illness within 3 to 7 days. The signs may include lethargy, vomiting, fever, and diarrhea (usually bloody). Generally, the first sign of CPV is lethargy. Secondary signs are a loss of appetite or diarrhea followed by vomiting. Diarrhea and vomiting result in dehydration that upsets the electrolyte balance and this may affect the dog critically. Secondary infections occur as a result of the weakened immune system. Because the normal intestinal lining is also compromised, blood and protein leak into the intestines leading to anemia and loss of protein, and endotoxins escaping into the bloodstream, causing endotoxemia. Dogs have a distinctive odor in the later stages of the infection. The white blood cell level falls, further weakening the dog. Any or all of these factors can lead to shock and death.
Diagnosis
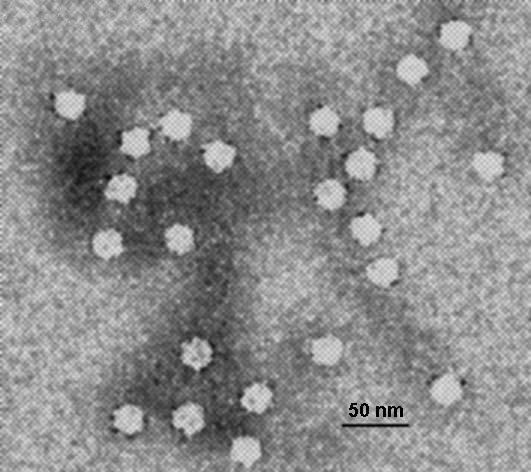
Diagnosis is made through detection of CPV2 in the feces by either an ELISA or a hemagglutination test, or by electron microscopy. PCR has become available to diagnose CPV2, and can be used later in the disease when potentially less virus is being shed in the feces that may not be detectable by ELISA. Clinically, the intestinal form of the infection can sometimes be confused with coronavirus or other forms of enteritis. Parvovirus, however, is more serious and the presence of bloody diarrhea, a low white blood cell count, and necrosis of the intestinal lining also point more towards parvovirus, especially in an unvaccinated dog. The cardiac form is typically easier to diagnose because the symptoms are distinct.
Treatment

Survival rate depends on how quickly CPV is diagnosed, the age of the dog and how aggressive the treatment is. Treatment usually involves extensive hospitalization, due to the severe dehydration and damage to the intestines and bone marrow. A CPV test should be given as early as possible if CPV is suspected in order to begin early treatment and increase survival rate if the disease is found.
Treatment ideally also consists of crystalloid IV fluids and/or colloids (e.g., Hetastarch), antinausea injections (antiemetics) such as maropitant, metoclopramide, dolasetron, ondansetron and prochlorperazine, and broad-spectrum antibiotic injections such as cefazolin/enrofloxacin, ampicillin/enrofloxacin, metronidazole, timentin, or enrofloxacin. IV fluids are administered and antinausea and antibiotic injections are given subcutaneously, intramuscularly, or intravenously. The fluids are typically a mix of a sterile, balanced electrolyte solution, with an appropriate amount of B-complex vitamins, dextrose and potassium chloride. Analgesic medications can be used to counteract the intestinal discomfort caused by frequent bouts of diarrhea; however, the use of opioid analgesics can result in secondary ileus and decreased motility.

In addition to fluids given to achieve adequate rehydration, each time the puppy vomits or has diarrhea in a significant quantity, an equal amount of fluid is administered intravenously. The fluid requirements of a patient are determined by the animal's body weight, weight changes over time, degree of dehydration at presentation and surface area.
A blood plasma transfusion from a donor dog that has already survived CPV is sometimes used to provide passive immunity to the sick dog. Some veterinarians keep these dogs on site, or have frozen serum available. There have been no controlled studies regarding this treatment. Additionally, fresh frozen plasma and human albumin transfusions can help replace the extreme protein losses seen in severe cases and help assure adequate tissue healing. However, this is controversial with the availability of safer colloids such as Hetastarch, as it will also increase the colloid osmotic pressure without the ill effect of predisposing that canine patient to future transfusion reaction.
Once the dog can keep fluids down, the IV fluids are gradually discontinued, and very bland food slowly introduced. Oral antibiotics are administered for a number of days depending on the white blood cell count and the patient's ability to fight off secondary infection. A puppy with minimal symptoms can recover in 2 or 3 days if the IV fluids are begun as soon as symptoms are noticed and the CPV test confirms the diagnosis. If more severe, depending on treatment, puppies can remain ill from 5 days up to 2 weeks. However, even with hospitalization, there is no guarantee that the dog will be cured and survive.
Unconventional treatments
There have been anecdotal reports of oseltamivir (Tamiflu) reducing disease severity and hospitalization time in canine parvovirus infection. The drug may limit the ability of the virus to invade the crypt cells of the small intestine and decrease gastrointestinal bacteria colonization and toxin production. However, due to the viral DNA replication pattern of parvovirus and the mechanism of action of oseltamivir, this medication has not shown to improve survival times or shorten hospitalization stay. Lastly, recombinant feline interferon omega (rFeIFN-ω), produced in silkworm larvae using a baculovirus vector, has been demonstrated by multiple studies to be an effective treatment. However, this therapy is not currently approved in the United States.
An unpublished 2012 study from Colorado State University showed good results with an intensive at-home treatment using maropitant (Cerenia) and Convenia (a long acting antibiotic injection), two drugs released by Zoetis (formerly Pfizer). This treatment was based on outpatient care, and would cost $200 to $300, a fraction of the $1,500 to $3,000 that inpatient care cost. However, the more-effective care is intravenous (IV) fluid therapy. In the CSU study, survival rate for the new treatment group was 85%, compared to the 90% survival for the conventional inpatient treatment. Note that the outpatient dogs received initial intravenous fluid resuscitation, and had aggressive subcutaneous fluid therapy and daily monitoring by a veterinarian.
History
Parvovirus CPV2 is a relatively new disease that appeared in the late 1970s. It was first recognized in 1978 and spread worldwide in one to two years. The virus is very similar to feline panleukopenia (also a parvovirus); they are 98% identical, differing only in two amino acids in the viral capsid protein VP2. It is also highly similar to mink enteritis, and the parvoviruses of raccoons and foxes. It is possible that CPV2 is a mutant of an unidentified parvovirus (similar to feline parvovirus (FPV)) of some wild carnivore. A strain of CPV2b (strain FP84) has been shown to cause disease in a small percentage of domestic cats, although vaccination for FPV seems to be protective. CPV2, however, does not cause disease in cats and does so only mildly in mink and raccoons, and is a virus almost exclusively affecting canines.
Two more strains of canine parvovirus CPV2a and CPV2b were identified in 1979 and 1984 respectively. Most cases of canine parvovirus infection are believed to be caused by these two strains, which have replaced the original strain, and the present day virus is different from the one originally discovered although they are indistinguishable by most routine tests. A third type, CPV2c (a Glu-426 mutant), has been discovered in Italy, Vietnam, and Spain.
Pathophysiology
There are two forms of CPV2: intestinal and cardiac. Puppies are most susceptible, but more than 80 percent of adult dogs show no symptoms. With severe disease, dogs can die within 48 to 72 hours without treatment by fluids. In the more common, less severe form, mortality is about 10 percent. Certain breeds, such as Rottweilers, Doberman Pinschers, and Pit bull terriers as well as other black and tan colored dogs may be more susceptible to CPV2. Along with age and breed, factors such as a stressful environment, concurrent infections with bacteria, parasites, and canine coronavirus increase a dog's risk of severe infection. Dogs who catch Parvovirus usually die from the dehydration it causes or secondary infection rather than the virus itself.
Intestinal form
Dogs become infected through oral contact with CPV2 in feces, infected soil, or fomites that carry the virus. Following ingestion, the virus replicates in the lymphoid tissue in the throat, and then spreads to the bloodstream. From there, the virus attacks rapidly dividing cells, notably those in the lymph nodes, intestinal crypts, and the bone marrow. There is depletion of lymphocytes in lymph nodes and necrosis and destruction of the intestinal crypts. Anaerobic bacteria that normally reside in the intestines can then cross into the bloodstream, a process known as translocation, with bacteremia leading to sepsis. The most common bacteria involved in severe cases are Clostridium, Campylobacter and Salmonella species. This can lead to a syndrome known as systemic inflammatory response syndrome (SIRS). SIRS leads to a range of complications such as hypercoagulability of the blood, endotoxaemia and acute respiratory distress syndrome (ARDS). Bacterial myocarditis has also been reported secondarily to sepsis. Dogs with CPV are at risk of intussusception, a condition where part of the intestine prolapses into another part. Three to four days following infection, the virus is shed in the feces for up to three weeks, and the dog may remain an asymptomatic carrier and shed the virus periodically. The virus is usually more deadly if the host is concurrently infested with worms or other intestinal parasites.
Cardiac form
This form is less common and affects puppies infected in the uterus or shortly after birth until about 8 weeks of age. The virus attacks the heart muscle and the puppy often dies suddenly or after a brief period of breathing difficulty due to pulmonary edema. On the microscopic level, there are many points of necrosis of the heart muscle that are associated with mononuclear cellular infiltration. The formation of excess fibrous tissue (fibrosis) is often evident in surviving dogs. Myofibers are the site of viral replication within cells. The disease may or may not be accompanied with the signs and symptoms of the intestinal form. However, this form is now rarely seen due to widespread vaccination of breeding dogs.
Even less frequently, the disease may also lead to a generalized infection in neonates and cause lesions and viral replication and attack in other tissues other than the gastrointestinal tissues and heart, but also brain, liver, lungs, kidneys, and adrenal cortex. The lining of the blood vessels are also severely affected, which lead the lesions in this region to hemorrhage.
Infection of the fetus
This type of infection can occur when a pregnant female dog is infected with CPV2. The adult may develop immunity with little or no clinical signs of disease. The virus may have already crossed the placenta to infect the fetus. This can lead to several abnormalities. In mild to moderate cases the pups can be born with neurological abnormalities such as cerebellar hypoplasia.
Virology
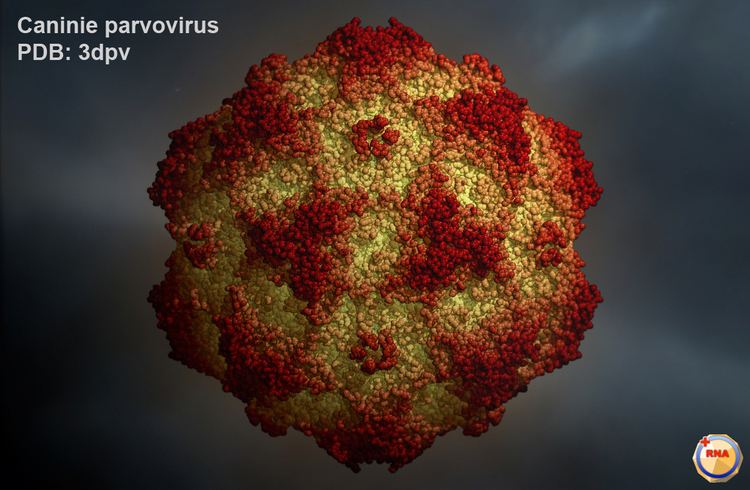
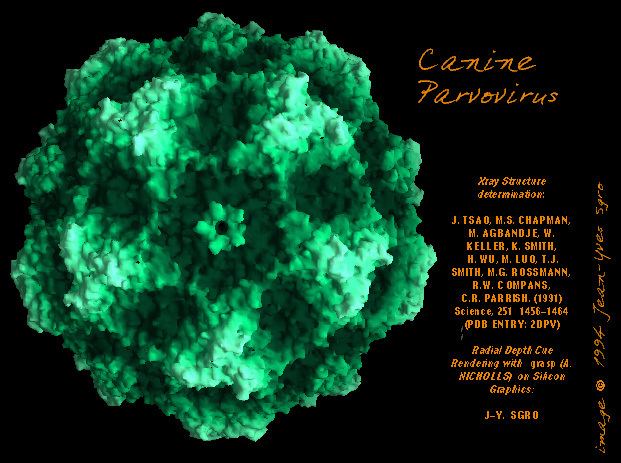
CPV2 is a non-enveloped single-stranded DNA virus. The name comes from the Latin parvus, meaning small, as the virus is only 20 to 26 nm in diameter. It has an icosahedral symmetry. The genome is about 5000 nucleotides long. CPV2 continues to evolve, and the success of new strains seems to depend on extending the range of hosts affected and improved binding to its receptor, the canine transferrin receptor. CPV2 has a high rate of evolution, possibly due to a rate of nucleotide substitution that is more like RNA viruses such as Influenzavirus A. In contrast, FPV seems to evolve only through random genetic drift.
CPV2 affects dogs, wolves, foxes, and other canids. CPV2a and CPV2b have been isolated from a small percentage of symptomatic cats and is more common than feline panleukopenia in big cats.
Previously it has been thought that the virus does not undergo cross species infection. However studies in Vietnam have shown that CPV2 can undergo minor antigenic shift and natural mutation to infect felids. Analyses of feline parvovirus (FPV) isolates in Vietnam and Taiwan revealed that more than 80% of the isolates were of the canine parvovirus type, rather than feline panleukopenia virus (FPLV). CPV2 may spread to cats easier than dogs and undergo faster rates of mutation within that species.
Variants
There are two types of canine parvovirus called canine minute virus (CPV1) and CPV2. CPV2 causes the most serious disease and affects domesticated dogs and wild canids. There are variants of CPV type 2 called CPV-2a, CPV-2b and CPV-2c. The antigenic patterns of 2a and 2b are quite similar to the original CPV type 2. Variant 2c however has a unique pattern of antigenicity. This has led to claims of ineffective vaccination of dogs, but studies have shown that the existing CPV vaccines based on CPV type 2b, provide adequate levels of protection against CPV type 2c.
Prevention and decontamination
Prevention is the only way to ensure that a puppy or dog remain healthy because the disease is extremely virulent and contagious. Appropriate vaccination should be performed starting at 7–8 weeks of age, with a booster given every 3–4 weeks until at least 16 weeks of age. Likewise, pregnant mothers should not be vaccinated as it will abort the puppies and could make the mother extremely sick. The virus is extremely hardy and has been found to survive in feces and other organic material such as soil for over 10 years. It survives extremely low and high temperatures. The only household disinfectant that kills the virus is bleach. The dilute bleach solution needs to be a (1:10 ratio) to disinfect and kill parvovirus.
Puppies are generally vaccinated in a series of doses, extending from the earliest time that the immunity derived from the mother wears off until after that passive immunity is definitely gone. Older puppies (16 weeks or older) are given 3 vaccinations 3 to 4 weeks apart. The duration of immunity of vaccines for CPV2 has been tested for all major vaccine manufacturers in the United States and has been found to be at least three years after the initial puppy series and a booster 1 year later.
A dog that successfully recovers from CPV2 generally remains contagious for up to three weeks, but it is possible they may remain contagious for up to six. Ongoing infection risk is primarily from fecal contamination of the environment due to the virus's ability to survive many months in the environment. Neighbours and family members with dogs should be notified of infected animals so that they can ensure that their dogs are vaccinated or tested for immunity. The vaccine will take up to 2 weeks to reach effective levels of immunity; the contagious individual should remain in quarantine until other animals are protected.