
Specialty medical genetics ICD-9-CM 759.89 MedlinePlus 000504 | ICD-10 Q87.8 DiseasesDB 454 | |
 | ||
OMIM 301050 104200 203780 300195 | ||
Alport syndrome is a genetic disorder affecting around 1 in 50,000 children, characterized by glomerulonephritis, end-stage kidney disease, and hearing loss. Alport syndrome can also affect the eyes, though the changes do not usually affect sight, except when changes to the lens occur in later life. Blood in urine is universal. Proteinuria is a feature as kidney disease progresses.
Contents
- Signs and symptoms
- Hematuria and proteinuria
- Hearing loss
- Leiomyomatosis
- Eye changes
- Other abnormalities
- Genetics
- Inheritance patterns
- Diagnosis
- Biopsy of kidneys or skin
- Family history
- Genetic testing
- Other tests
- Kidney disease and renal failure
- Prognosis
- References
The disorder was first identified in a British family by University of Edinburgh Medical School graduate Cecil A. Alport in 1927,. Alport Syndrome once also had the label hereditary nephritis, but this is misleading as there are many other causes of hereditary kidney disease and 'nephritis'.
Alport syndrome is caused by an inherited defect in type IV collagen—a structural material that is needed for the normal function of different parts of the body. Since type IV collagen is found in the ears, eyes, and kidneys, this explains why Alport syndrome affects different seemingly unrelated parts of the body (ears, eyes, kidneys, etc.).
Signs and symptoms
These descriptions refer to 'classic' Alport Syndrome, which usually causes significant disease from young adult or late childhood life. Some individuals, usually with milder mutations or 'carrier' status, develop disease later, or show only some of the features of classic disease.
Hematuria and proteinuria
Blood in urine is a usual feature of Alport Syndrome from early infancy, identifiable on urine dipsticks. In young children, episodes of visible (macroscopic) haematuria may occur. Protein begins to appear in urine as the disease progresses. This is now regarded as an indication for treatment with ACE inhibitors.
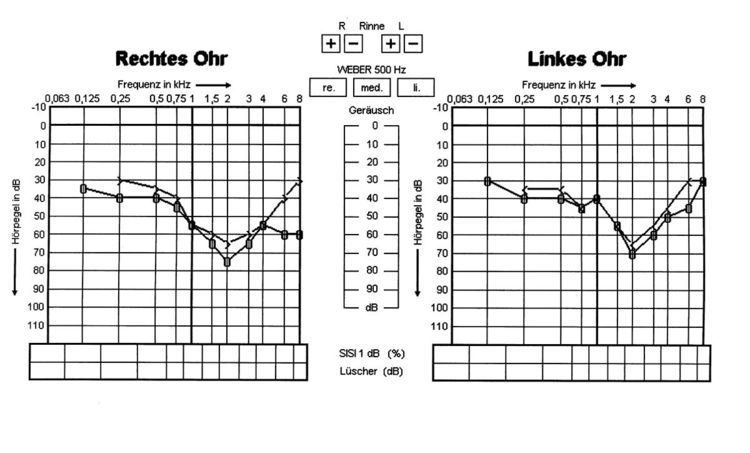
Hearing loss
Alport syndrome can also cause hearing loss although some patients are not affected. Hearing in Alport syndrome patients is normal at birth. Hearing loss in affected patients develops progressively, usually at the stage when kidney function is normal, but there is substantial proteinuria. However, in some patients, hearing loss is only noted after kidney function has been lost. Characteristically the early changes are reduced abililty to hear high frequency sounds, 'high-tone hearing loss'. This becomes more severe and affects lower frequencies too. Hearing loss is not usually complete in Alport Syndrome, good communication is almost always possible with the use of hearing aids.
Leiomyomatosis
Diffuse leiomyomatosis of the esophagus and tracheobronchial tree has been reported in some families with Alport syndrome. Symptoms usually appear in late childhood and include dysphagia, postprandial vomiting, substernal or epigastric pain, recurrent bronchitis, dyspnea, cough, and stridor. Leiomyomatosis is confirmed by computed tomography (CT) scanning or magnetic resonance imaging (MRI).
Eye changes
Various eye abnormalities are often seen including lenticonus, kerataconus, cataracts as well as retinal flecks in the macula and mid-periphery. These rarely threaten vision. Lenticonus (cone-shaped lens) can be treated by replacement of the lens, as for cataracts. Mild kerataconus can be treated with hard or piggy-back contact lenses, severe cases may require a corneal transplant.
Other abnormalities
Aortic dissection has been described very rarely in patients with early-onset disease. Leiomyomas, tumours of smooth muscle affecting the oesophagus and female genital tract, may occur in a rare overlap syndrome involving the adjacent COL4A5 and COL4A6 genes.
Genetics
Alport syndrome is caused by mutations in COL4A3, COL4A4, and COL4A5, three of six human genes involved in basement membrane (type IV) collagen biosynthesis. Mutations in any of these genes prevent the proper production or assembly of the specialised type IV collagen '345' network found in the glomerulus, which is an important structural component of basement membranes in the kidney, inner ear, and eye. It is also found in other locations, including the alveoli of the lungs. Basement membranes are thin, sheet-like structures that separate and support cells in many tissues. Type IV collagen '112' type is found in both vertebrates and invertebrates, and is the major isoform in most human basement membranes. When mutations prevent the formation of 345 type IV collagen network in the glomerulus, the 112 network, which is formed in fetal development but usually replaced by 345, persists into adult life.
Inheritance patterns
Alport syndrome can have different inheritance patterns depending on which specific mutation is present.
Clinical utility gene card for: Alport syndrome.
Diagnosis
The diagnosis can usually be made on a combination of clinical, family history and biopsy criteria.
Biopsy of kidneys or skin
To be helpful, kidney biopsies need to be taken before the disease is too advanced. Changes on conventional (light) microscopy are not characteristic, and the possibility of other diagnoses, particularly focal segmental glomerulosclerosis (FSGS) may be raised. Electron microscopy shows a characteristic sequence of changes from thinning of the glomerular basement membrane (GBM), developing into areas of thinning and thickening, and finally into a complex appearance with apparent splitting, often described as a 'basketweave' appearance. Early or very localised changes on this spectrum are not diagnostic, but the later changes are considered diagnostic.
Immunohistochemistry or immunofluorescence studies to identify the COL3-4-5 proteins in GBM can be helpful. However these studies may be normal in some patients with Alport syndrome, especially milder variants.
Skin contains type IV collagen in a '556' network. Skin biopsies have been used to show absence of the COL4A5 gene product, but these techniques are not straightforward, only apply to patients with severe COL4A5 mutations, and are not widely available. Genetic testing is now a better alternative if kidney biopsy is not possible.
Family history
A family history of end stage renal disease with hearing impairment is suggestive of Alport syndrome, but other conditions can cause this combination of abnormalities. Most can be distinguished by clinical features. The finding of haematuria in relatives is suggestive. While X-linked inheritance is the most common pattern, genetic testing is revealing that atypical presentations may be more common than currently thought.
Genetic testing
Genetic testing plays an increasingly important role in confirming the diagnosis where the clinical features do not amount to proof.
Other tests
The use of eye examinations for screening has been proposed.
Kidney disease and renal failure
In addition to measures for chronic kidney disease (CKD) of any cause, there is evidence that ACE inhibitors can slow the deterioration of kidney function in Alport Syndrome, delaying the need for dialysis or transplantation. The development of proteinuria has been recommended as an indication for commencing treatment.
Once kidney failure has developed, patients usually do well on dialysis or with a kidney transplant. Very rarely the Alport molecule in the donor kidney causes an aggressive immune response in the recipient, 'Alport post-transplant anti-GBM disease'.
Gene therapy has been frequently discussed, but delivering it to the podocytes in the glomerulus that normally produce the type IV collagen in the glomerular basement membrane is challenging.
Hearing loss
It is not known whether ACE inhibitors or other treatments affect hearing loss. For those with classic Alport Syndrome, hearing aids are often required in teenage or young adult years.
Prognosis
Studies of the life expectancy of patients with Alport syndrome are rare, but one 2012 study of 456 male patients from across Europe who received a kidney transplant found that they had somewhat increased life expectancy compared to matched controls (the controls were "randomly selected from the same age, year, and modality categories").