
Specialty nephrology MedlinePlus 000478 | ICD-9-CM 581.1 eMedicine med/2944 | |
 | ||
ICD-10 N00-N08 (with .1 suffix) OMIM 603278 603965 607832 612551 613237 600995 | ||
Focal segmental glomerulosclerosis (FSGS) is a cause of nephrotic syndrome in children and adolescents, as well as a leading cause of kidney failure in adults. It is also known as "focal glomerular sclerosis" or "focal nodular glomerulosclerosis." It accounts for about a sixth of the cases of nephrotic syndrome. (Minimal change disease (MCD) is by far the most common cause of nephrotic syndrome in children: MCD and primary FSGS may have a similar cause.)
Contents
Appearance
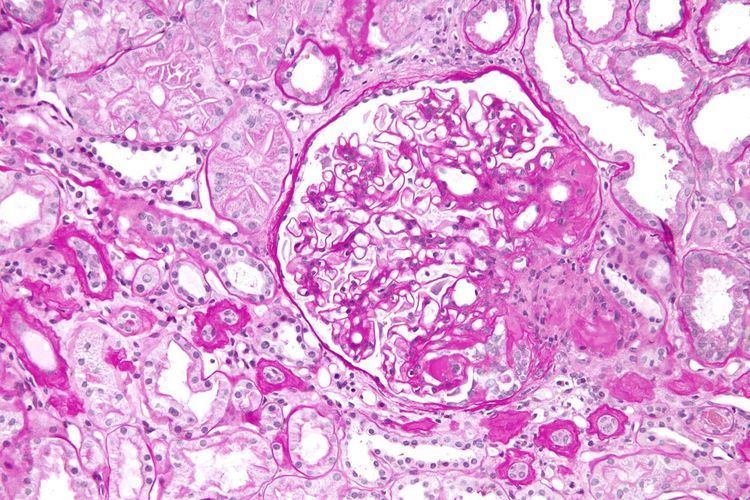
The individual components of the name refer to the appearance of the kidney tissue on biopsy: focal—only some of the glomeruli are involved (as opposed to diffuse), segmental—only part of each glomerulus is involved (as opposed to global), glomerulosclerosis—refers to scarring of the glomerulus (a part of the nephron (the functional unit of the kidney)). The glomerulosclerosis is usually indicated by heavy PAS staining and findings of immunoglobulin M (IgM) and C3-convertase (C3) in the sclerotic segment.
Classification
Depending on the cause it is broadly classified as:
There are many other classification schemes also.
Pathologic variants
Five mutually exclusive variants of focal segmental glomerulosclerosis may be distinguished by the pathologic findings seen on renal biopsy:
- Collapsing variant
- Glomerular tip lesion variant
- Cellular variant
- Perihilar variant
- Not otherwise specified (NOS) variant.
Recognition of these variants may have prognostic value in individuals with primary focal segmental glomerulosclerosis (i.e. where no underlying cause is identified). The collapsing variant is associated with higher rate of progression to end-stage renal disease, whereas glomerular tip lesion variant has a low rate of progression to end-stage renal disease in most patients. Cellular variant shows similar clinical presentation to collapsing and glomerular tip variant but has intermediate outcomes between these two variants. However, because collapsing and glomerular tip variant show overlapping pathologic features with cellular variant, this intermediate difference in clinical outcomes may reflect a sampling bias in cases of cellular focal segmental glomerulosclerosis (i.e. unsampled collapsing variant or glomerular tip variant). The prognostic significance of perihilar and NOS variants has not yet been determined. The NOS variant is the most common subtype. Collapsing variant is the most common type of glomerulopathy caused by HIV infection.
Causes
Some general secondary causes are listed below:
Focal segmental glomerulosclerosis may develop following acquired loss of nephrons from reflux nephropathy. Proteinuria is nonselective in most cases and may be in subnephrotic range (nephritic range <3.0gm/24hr) or nephritic range.
There are currently several known genetic causes of the hereditary forms of FSGS.
Some researchers found SuPAR as a cause of FSGS.
Symptoms and signs
In children and some adults, FSGS presents as a nephrotic syndrome, which is characterized by edema (associated with weight gain), hypoalbuminemia (low serum albumin, a protein in the blood), hyperlipidemia and hypertension (high blood pressure). In adults, it may also present as kidney failure and proteinuria, without a full-blown nephrotic syndrome.