
Specialty infectious disease ICD-9-CM 127.2 MedlinePlus 000630 | ICD-10 B78 DiseasesDB 12559 | |
 | ||
eMedicine article/999614-overview | ||
Strongyloidiasis is a human parasitic disease caused by the nematode (roundworm) called Strongyloides stercoralis, or sometimes S. fülleborni which is a type of helminth. It belongs to a group of nematodes called roundworms. This intestinal worm can cause a number of symptoms in people, principally skin symptoms, abdominal pain, diarrhea and weight loss. In some people, particularly those who require corticosteroids or other immunosuppressive medication, Strongyloides can cause a hyperinfection syndrome that can lead to death if untreated. The diagnosis is made by blood and stool tests. The medication ivermectin is widely used to treat strongyloidiasis.
Contents
Strongyloidiasis is a type of soil-transmitted helminthiasis. It is thought to affect 30–100 million people worldwide, mainly in tropical and subtropical countries. It belongs to the group of neglected tropical diseases, and worldwide efforts are aimed at eradicating the infection.
Signs and symptoms
Strongyloides infection occurs in five forms. On acquiring the infection, there may be respiratory symptoms (Löffler's syndrome). The infection may then become chronic with mainly digestive symptoms. On reinfection (when larvae migrate through the body), there may be respiratory, skin and digestive symptoms. Finally, the hyperinfection syndrome causes symptoms in many organ systems, including the central nervous system.
Uncomplicated disease
Frequently asymptomatic. Gastrointestinal system symptoms include abdominal pain and diarrhea. Pulmonary symptoms (including Löffler's syndrome) can occur during pulmonary migration of the filariform larvae. Dermatologic manifestations include urticarial rashes in the buttocks and waist areas as well as larva currens. Eosinophilia is generally present.
Strongyloidiasis can become chronic and then become completely asymptomatic.
Disseminated disease
Disseminated strongyloidiasis occurs when patients with chronic strongyloidiasis become immunosuppressed. It presents with abdominal pain, distension, shock, pulmonary and neurologic complications and septicemia, and is potentially fatal. The worms enter the bloodstream from the bowel wall, simultaneously allowing entry of bowel bacteria such as Escherichia coli. This may cause symptoms such as sepsis (bloodstream infection), and the bacteria may spread to other organs where they may cause localized infection such as meningitis.
Dissemination can occur many decades after the initial infection and has been associated with high dose corticosteroids, organ transplant, HIV, lepromatous leprosy, tertiary syphilis, aplastic anemia, malnutrition, advanced tuberculosis and radiation poisoning. It is often recommended that patients being started on immunosuppression be screened for chronic strongyloidiasis; however, this is often impractical (screen tests are often unavailable) and in developed countries, the prevalence of chronic strongyloidiasis is very small, so screening is usually not cost-effective, except in endemic areas.
It is important to note that there is not necessarily any eosinophilia in the disseminated disease. Absence of eosinophilia may indicate poor prognosis.
Diagnosis
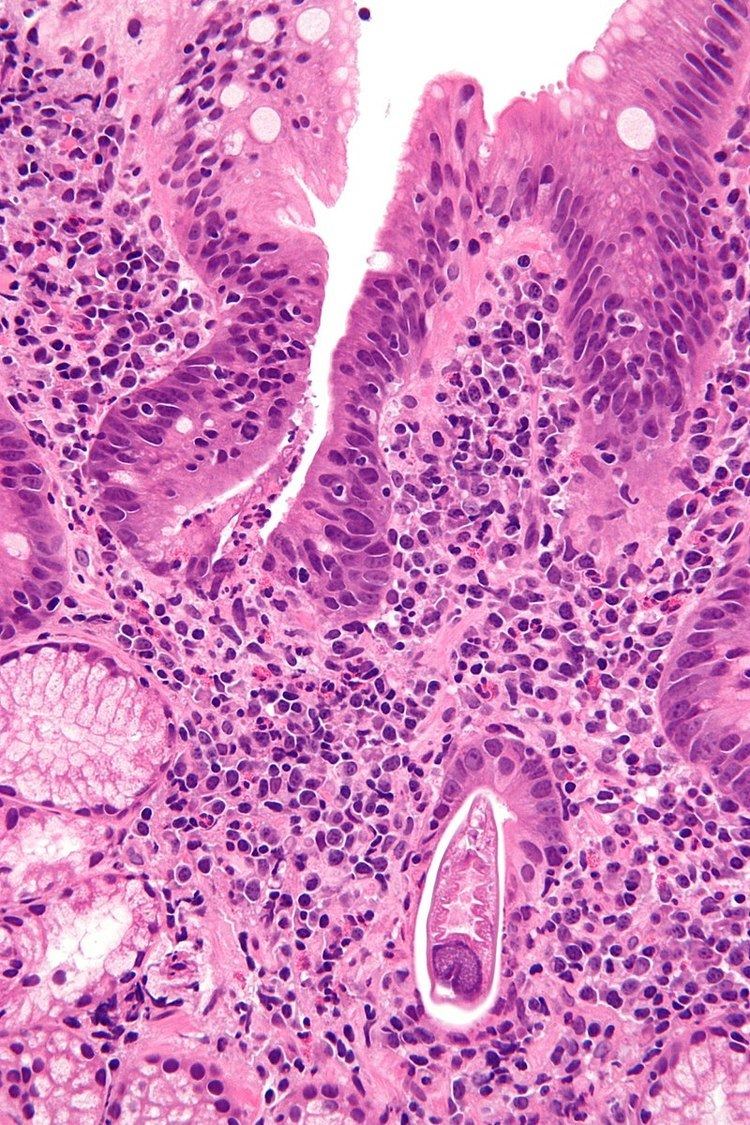
Diagnosis rests on the microscopic identification of larvae (rhabditiform and occasionally filariform) in the stool or duodenal fluid. Examination of many samples may be necessary, and not always sufficient, because direct stool examination is relatively insensitive, with a single sample only able to detect larvae in about 25% of cases. It can take 4 weeks from initial infection to the passage of larvae in the stool.
The stool can be examined in wet mounts:
Culture techniques are the most sensitive, but are not routinely available in the West. In the UK, culture is available at either of the Schools of Tropical Medicine in Liverpool or London. Direct examination must be done on stool that is freshly collected and not allowed to cool down, because hookworm eggs hatch on cooling and the larvae are very difficult to distinguish from Strongyloides.
Finding Strongyloides in the stool is negative in up to 70% of tests. It is important to undergo frequent stool sampling as well as duodenal biopsy if a bad infection is suspected. The duodenal fluid can be examined using techniques such as the Enterotest string or duodenal aspiration. Larvae may be detected in sputum from patients with disseminated strongyloidiasis.
Given the poor ability of stool examination to diagnose strongyloides, detecting antibodies by ELISA can be useful. Serology can cross-react with other parasites, remain positive for years after successful treatment or be falsely negative in immunocompromised patients. Infected patients will also often have an elevated eosinophil count, with an average of absolute eosinophil count of 1000 in one series. The combination of clinical suspicion, a positive antibody and a peripheral eosinophilia can be strongly suggestive of infection.
Treatment
The drug of choice for the treatment of uncomplicated strongyloidiasis is ivermectin. Ivermectin does not kill the Strongyloides larvae, only the adult worms, therefore repeat dosing may be necessary to properly eradicate the infection. There is an auto-infective cycle of roughly two weeks in which Ivermectin should be re-administered however additional dosing may still be necessary as it will not kill Strongyloides in the blood or larvae deep within the bowels or diverticula. Other drugs that are effective are albendazole and thiabendazole (25 mg/kg twice daily for 5 days—400 mg maximum (generally)). All patients who are at risk of disseminated strongyloidiasis should be treated. The optimal duration of treatment for patients with disseminated infections is not clear.
Treatment of strongyloidiasis can be difficult and Strongyloides has been known to live in individuals for decades; even after treatment. Continued treatment is thus necessary even if symptoms resolve.
Because of the high cost of Stromectol, the veterinary formula Ivomec can be used. Government programs are needed to help citizens finance lifelong medication.
Clothes and sheets must be washed with enzyme washing powder and dried on hot daily.
History
The disease was first recognized in 1876 by the French physician Louis Alexis Normand, working in the naval hospital in Toulon; he identified the adult worms, and sent them to Arthur Réné Jean Baptiste Bavay, chief inspector for health, who observed that these were the adult forms of the larvae found in the stool. In 1883 the German parasitologist Rudolf Leuckart made initial observations on the life cycle of the parasite, and Belgian physician Paul Van Durme (building on observations by the German parasitologist Arthur Looss) described the mode of infection through the skin. The German parasitologist Friedrich Fülleborn described autoinfection and the way by which strongyloidiasis involves the intestine. Interest in the condition increased in the 1940s when it was discovered that those who had acquired the infection abroad and then received immunosuppression developed hyperinfestation syndrome.