
TA A14.2.07.023 | Latin nervus saphenus FMA 45262 | |
 | ||
The saphenous nerve (long or internal saphenous nerve) is the largest cutaneous branch of the femoral nerve. It is a strictly sensory nerve, and has no motor function.
Contents
Structure
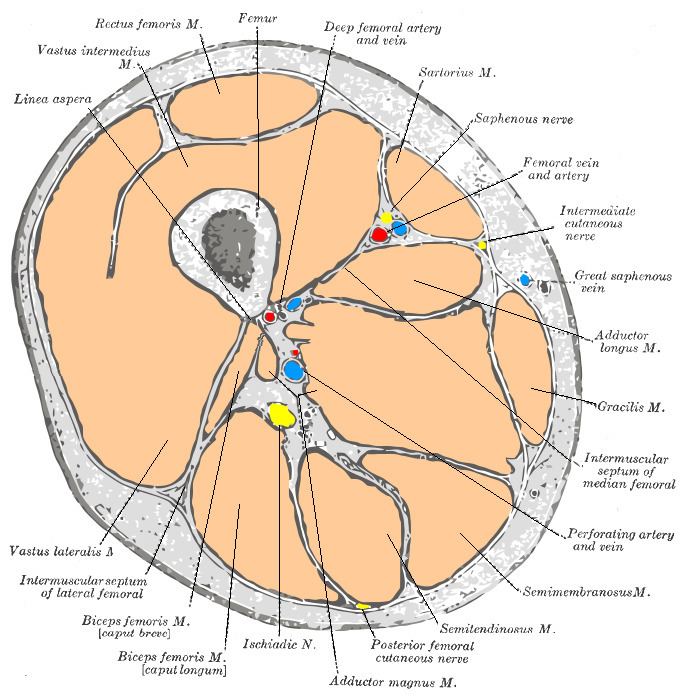
It approaches the femoral artery where this vessel passes beneath the sartorius, and lies in front of the artery, behind the aponeurotic covering of the adductor canal, as far as the opening in the lower part of the Adductor magnus.
Here it diverges from the artery, and emerges from behind the lower edge of the aponeurotic covering of the canal; it descends vertically along the medial side of the knee behind the sartorius, pierces the fascia lata, between the tendons of the Sartorius and Gracilis, and becomes subcutaneous.
The nerve then passes along the tibial side of the leg, accompanied by the great saphenous vein, descends behind the medial border of the tibia, and, at the lower third of the leg, divides into two branches:
Function
The saphenous nerve, about the middle of the thigh, gives off a branch which joins the subsartorial plexus.
At the medial side of the knee it gives off a large infrapatellar branch, which pierces the sartorius and fascia lata, and is distributed to the skin in front of the patella.
Below the knee, the branches of the saphenous nerve (medial crural cutaneous branches) are distributed to the skin of the front and medial side of the leg, communicating with the cutaneous branches of the femoral, or with filaments from the obturator nerve.
Clinical Significance
Procedures such as saphenous vein cutdown or orthopedic surgery that includes incisions or dissection over the distal tibia or medial malleolus can result in damage to the saphenous nerve, resulting in loss of cutaneous sensation in the medial leg. This is due to the intimate path that the saphenous nerve and the great saphenous vein travel. The saphenous nerve is also often damaged during vein harvest for bipass surgery and during trochanter placement during knee arthroscopy. There appears to be occasional meaningful individual variation in the pathway of this nerve, such that the illustration of it done for Gray's Anatomy, for example, likely represents an unusual rather than usual course.
The saphenous nerve can experience entrapment syndrome from exercises involving the quadriceps or from prolonged walking or standing. It is characterized by a burning sensation in most patients. Pain often occurs at night, long after the physical exercise which induced it has stopped, and may be aggravated by climbing stairs. Usually, in this case, motor function of the lower leg will not be impaired. This is a key distinction between saphenous nerve neuropathy and lower back radiculopathy. Saphenous nerve neuropathy only demonstrates sensory alterations, while lumbar radiculopathy will affect the motor, sensory, and deep tendon reflexes of the lower leg.