
Latin tarsus TA A01.1.00.041 | MeSH A02.835.583.378.062 FMA 9665 | |
 | ||
The ankle, or the talocrural region, is the region where the foot and the leg meet. The ankle includes three joints: the ankle joint proper or talocrural joint, the subtalar joint, and the inferior tibiofibular joint. The movements produced at this joint are dorsiflexion and plantarflexion of the foot. In common usage, the term ankle refers exclusively to the ankle region. In medical terminology, "ankle" (without qualifiers) can refer broadly to the region or specifically to the talocrural joint.
Contents
The main bones of the ankle region are the talus (in the foot), and the tibia and fibula (in the leg). The talocrural joint is a synovial hinge joint that connects the distal ends of the tibia and fibula in the lower limb with the proximal end of the talus. The articulation between the tibia and the talus bears more weight than that between the smaller fibula and the talus.
Bones
The bony architecture of the ankle consists of three bones: the tibia, the fibula, and the talus. The articular surface of the tibia is referred to as the plafond. The medial malleolus is a bony process extending distally off the medial tibia. The distal-most aspect of the fibula is called the lateral malleolus. Together, the malleoli, along with their supporting ligaments, stabilize the talus underneath the tibia.
The bony arch formed by the tibial plafond and the two malleoli is referred to as the ankle "mortise" (or talar mortise). The mortise is a rectangular socket. The ankle is composed of three joints: the talocrural joint (also called talotibial joint, tibiotalar joint, talar mortise, talar joint), the subtalar joint (also called talocalcaneal), and the Inferior tibiofibular joint. The joint surface of all bones in the ankle are covered with articular cartilage.
The distances between the bones in the ankle are as follows:
Decreased distances indicate osteoarthritis.
Ligaments
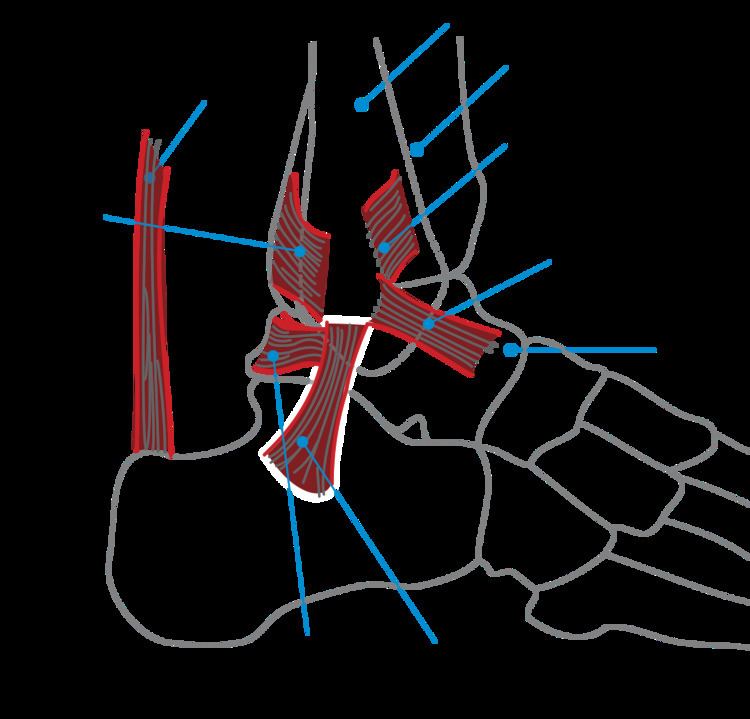
The ankle joint is bound by the strong deltoid ligament and three lateral ligaments: the anterior talofibular ligament, the posterior talofibular ligament, and the calcaneofibular ligament.
Though it does not span across the ankle joint itself, the syndesmotic ligament makes an important contribution to the stability of the ankle. This ligament spans the syndesmosis, i.e. the articulation between the medial aspect of the distal fibula and the lateral aspect of the distal tibia. An isolated injury to this ligament is often called a high ankle sprain.
The bony architecture of the ankle joint is most stable in dorsiflexion. Thus, a sprained ankle is more likely to occur when the ankle is plantar-flexed, as ligamentous support is more important in this position. The classic ankle sprain involves the anterior talofibular ligament (ATFL), which is also the most commonly injured ligament during inversion sprains. Another ligament that can be injured in a severe ankle sprain is the calcaneofibular ligament.
Mechanoreceptors
Mechanoreceptors of the ankle send proprioceptive sensory input to the central nervous system (CNS). Muscle spindles are thought to be the main type of mechanoreceptor responsible for proprioceptive attributes from the ankle. The muscle spindle gives feedback to the CNS system on the current length of the muscle it innervates and to any change in length that occurs.
It was hypothesized that muscle spindle feedback from the ankle dorsiflexors played the most substantial role in proprioception relative to other muscular receptors that cross at the ankle joint. However, due to the multi-planar range of motion at the ankle joint there is not one group of muscles that is responsible for this. This helps to explain the relationship between the ankle and balance.
In 2011, a relationship between proprioception of the ankle and balance performance was seen in the CNS. This was done by using a fMRI machine in order to see the changes in brain activity when the receptors of the ankle are stimulated. This implicates the ankle directly with the ability to balance. Further research is needed in order to see to what extent does the ankle affect balance.
Function
Dorsiflexion due to actions of Tibialis Anterior and Extensor hallucis longus muscles
Plantarflexion due to actions of Gastrocnemius, Soleus and Plantaris muscles
Fractures
Symptoms of an ankle fracture can be similar to those of ankle sprains (pain), though typically they are often more severe by comparison. It is exceedingly rare for the ankle joint to dislocate in the presence of ligamentous injury alone.
The talus is most commonly fractured by two methods. The first is hyperdorsiflexion, where the neck of the talus is forced against the tibia and fractures. The second is jumping from a height - the body is fractured as the talus transmits the force from the foot to the lower limb bones.
In the setting of an ankle fracture the talus can become unstable and subluxate or dislocate. People may complain of ecchymosis (bruising), or there may be an abnormal position, abnormal motion, or lack of motion. Diagnosis is typically by X-ray. Treatment is either via surgery or casting depending on the fracture types.
Imaging
The initial evaluation of suspected ankle pathology is usually by radiograph, with the three major anatomic landmarks for ligamentous injury. The first is the tibiofibular clear space, the horizontal distance from the lateral border of the posterior tibial malleolus to the medial border of the fibula, with greater than 5 mm being abnormal. The second is tibiofibular overlap, the horizontal distance between the medial border of the fibula and the lateral border of the anterior tibial prominence, with less than 10 mm being abnormal. The final measurement is the medial clear space, the distance between the lateral aspect of the medial malleolus and the medial border of the talus at the level of the talar dome, with a measurement greater than 4 mm being abnormal. Loss of any of these normal anatomic spaces can indirectly reflect ligamentous injury or occult fracture, and can be followed by MRI or CT.
History
The word ankle or ancle is common, in various forms, to Germanic languages, probably connected in origin with the Latin angulus, or Greek αγκυλος, meaning bent.
Evolution
It has been suggested that dexterous control of toes has been lost in favour of a more precise voluntary control of the ankle joint.