
Pronunciation /ˌnɛɡlərˈaɪəsɪs/ ICD-10 A06.6, B60.2 | Specialty Infectious disease ICD-9-CM 136.2 | |
 | ||
Synonyms primary amoebic meningoencephalitis (PAM), amebic encephalitis, naegleria infection, amoebic meningitis | ||
Naegleriasis (also known as primary amoebic meningoencephalitis) is an infection of the brain by the free-living unicellular Naegleria fowleri.
Contents
- Signs and symptoms
- Cause
- Pathogenesis
- Diagnosis
- Prevention
- Treatment
- Epidemiology
- History
- Society and culture
- Research
- References
N. fowleri is typically found in warm bodies of fresh water, such as ponds, lakes, rivers, and hot springs. It is also found in soil, poorly maintained municipal water supplies, water heaters, near warm-water discharges of industrial plants, and in poorly chlorinated, or unchlorinated swimming pools, in an amoeboid or temporary flagellate stage. There is no evidence of it living in salt water.
Although infection occurs rarely, it nearly always results in death, with a case fatality rate greater than 95%.
Signs and symptoms
Onset symptoms of infection can start from one to seven days after exposure. Initial symptoms include changes in taste and smell, headache, fever, nausea, vomiting, and a stiff neck. Secondary symptoms include confusion, hallucinations, lack of attention, ataxia, and seizures. After the start of symptoms, the disease progresses rapidly over three to seven days, with death occurring usually from seven to fourteen days later, although it can take longer. In 2013, a man in Taiwan died twenty-five days after being infected by Naegleria fowleri.
It affects healthy children or young adults with no prior history of immune compromise who have recently been exposed to bodies of fresh water.
Cause
N. fowleri invades the central nervous system via the nose, specifically through the olfactory mucosa of the nasal tissues. This usually occurs as the result of the introduction of water that has been contaminated with N. fowleri into the nose during activities such as swimming, bathing, or nasal irrigation.
The amoeba follows the olfactory nerve fibers through the cribriform plate of the ethmoid bone into the skull. There, it migrates to the olfactory bulbs and subsequently other regions of the brain, where it feeds on the nerve tissue, resulting in significant necrosis and bleeding.
The organism then begins to consume cells of the brain, piecemeal, by means of an amoebostome, a unique actin-rich, sucking apparatus extended from its cell surface. It then becomes pathogenic, causing primary amoebic meningoencephalitis (PAM or PAME).
Pathogenesis
Naegleria fowleri propagates in warm, stagnant bodies of freshwater (typically during the summer months), and enters the central nervous system after insufflation of infected water by attaching itself to the olfactory nerve. It then migrates through the cribriform plate and into the olfactory bulbs of the forebrain, where it multiplies itself greatly by feeding on nerve tissue.
Diagnosis
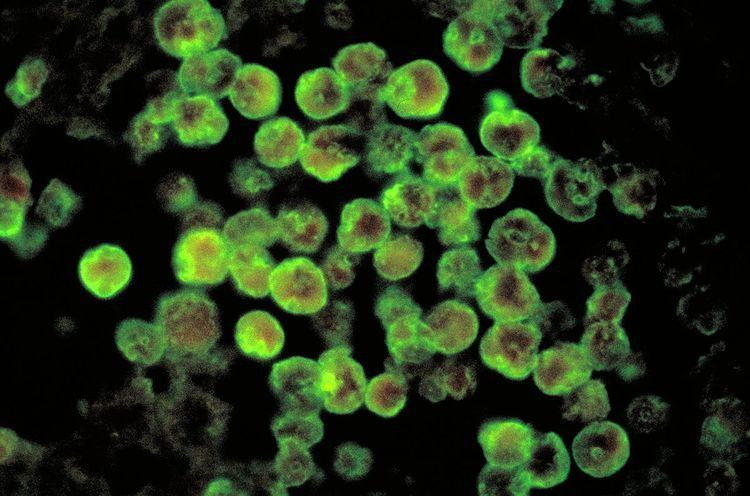
N. fowleri can be grown in several kinds of liquid axenic media or on non-nutrient agar plates coated with bacteria. Escherichia coli can be used to overlay the non-nutrient agar plate and a drop of cerebrospinal fluid sediment is added to it. Plates are then incubated at 37 °C and checked daily for clearing of the agar in thin tracks, which indicate the trophozoites have fed on the bacteria. Detection in water is performed by centrifuging a water sample with E. coli added, then applying the pellet to a non-nutrient agar plate. After several days, the plate is microscopically inspected and Naegleria cysts are identified by their morphology. Final confirmation of the species' identity can be performed by various molecular or biochemical methods. Confirmation of Naegleria presence can be done by a so-called flagellation test, where the organism is exposed to a hypotonic environment (distilled water). Naegleria, in contrast to other amoebae, differentiates within two hours into the flagellate state. Pathogenicity can be further confirmed by exposure to high temperature (42 °C): Naegleria fowleri is able to grow at this temperature, but the nonpathogenic Naegleria gruberi is not.
Prevention
Michael Beach, a recreational waterborne illness specialist for the Centers for Disease Control and Prevention, stated in remarks to the Associated Press that the wearing of nose-clips to prevent insufflation of contaminated water would be effective protection against contracting PAM, noting that "You'd have to have water going way up in your nose to begin with".
Treatment
Since its first description in the 1960s, only seven people worldwide have been reported to have survived PAM as of 2015, with three in the United States and one in Mexico. The prognosis remains poor for those who contract PAM, and survival remains less than 1%.
On the basis of the laboratory evidence and case reports, amphotericin B has been the traditional mainstay of PAM treatment since the first reported survivor in the US in 1982.
Treatment has often also used combination therapy with multiple other antimicrobials in addition to amphotericin such as fluconazole, miconazole, rifampicin and azithromycin. They have shown limited success only when administered early in the course of an infection. Fluconazole is commonly used as it has been shown to have synergistic effects against naegleria when used with amphotericin in-vitro.
While the use of rifampicin has been common, including in all four North American cases of survival, its continued use has been questioned. It only has variable activity in-vitro and it has strong effects on the therapeutic levels of other antimicrobials used by inducing cytochrome p450 pathways.
Steroids such as dexamethasone have also been used to try to reduce inflammation of the brain.
In 2013, the two most recent successfully treated cases in the US utilized drug combinations that included the medication miltefosine as well as targeted temperature management. There is currently no data on how well miltefosine is able to reach the central nervous system. The US CDC is currently offering miltefosine to doctors for the treatment of free-living ameobas including naegleria.
Untimely diagnoses remain a very significant impediment to the successful treatment of infection, as most cases have only been discovered post mortem. Infection killed 121 people in the United States from 1937 through 2007.
Epidemiology
The disease is rare and highly lethal: there have only been 300 cases as of 2008. Drug treatment research at Aga Khan University in Pakistan has shown that in-vitro drug susceptibility tests with some FDA approved drugs used for non-infectious diseases have proved to kill Naegleria fowleri with an amoebicidal rate greater than 95%. The same source has also proposed a device for drug delivery via the transcranial route to the brain.
This form of nervous system infection by amoeba was first documented in Australia in 1965. In 1966, four cases were reported in the USA. By 1968 the causative organism, previously thought to be a species of Acanthamoeba or Hartmannella, was identified as Naegleria. This same year, occurrence of 16 cases over a period of two years (1963–1965) was reported in Ústí nad Labem, Czechoslovakia. In 1970, the species of amoeba was named N. fowleri.
The number of cases of infection could increase due to climate change. In 2016 an infection was contracted in Maryland, four miles south of the Pennsylvania border; this was the northernmost North American case other than the three or four Minnesota cases from 2008 to 2015. Also, the numbers of reported cases are expected to show an increase, simply because of better informed diagnoses being made both in living patients and also in autopsy findings.
History
Australian Physicians Fowler and Carter first described human disease caused by amebo-flagellates in Adelaide in 1965. Their work on amebo-flagellates has provided an example of how a protozoan can effectively live both freely in the environment, and in a human host. Since 1965, more than 144 cases have been confirmed in different countries. In 1966, Fowler termed the infection resulting from N. fowleri, primary amoebic meningoencephalitis (PAM) to distinguish this central nervous system (CNS) invasion from other secondary invasions made by other amoebae such as Entamoeba histolytica. A retrospective study determined the first documented case of PAM possibly occurred in Britain in 1909.
The specific name, Naegleria Fowleri, were named for Mathieu Naegler (1867–1934), a French Parasitologist and Zoologist who discovered the species for the first time in 1899 and Malcolm Fowler (1924–1974), the Australian Doctor who described the distinct disease process of the pathogen in Australia in 1965.
Society and culture
Naegleria fowleri has also known as the "brain-eating amoeba". The term "brain-eating amoeba" has also been applied to Balamuthia mandrillaris, causing some confusion between the two, however Balamuthia mandrillaris is unrelated to Naegleria fowleri, and causes a different disease called granulomatous amoebic encephalitis, and unlike Naegleriasis, which is usually seen in people with normal immune function, granulomatous amoebic encephalitis is usually seen in people with poor immune function such as those with HIV/AIDS or leukemia.
Research
The U.S. National Institutes of Health had budgeted $800,000 for research on the disease in 2016.
Phenothiazines have been tested in vitro and in animal models of PAM.