
AHFS/Drugs.com Monograph License data US FDA: Modafinil | MedlinePlus a602016 | |
 | ||
Trade names Provigil, others (see below) Pregnancycategory AU: B3US: C (Risk not ruled out) Dependenceliability Psychological: Very lowPhysical: Negligible | ||
Modafinil (INN, USAN, BAN, JAN) is a wakefulness-promoting agent (or eugeroic) used for treatment of disorders such as narcolepsy, shift work sleep disorder, and excessive daytime sleepiness associated with obstructive sleep apnea. It has also seen widespread off-label use as a purported cognition-enhancing agent. In English-speaking countries it is sold under the brand names Alertec, Modavigil, and Provigil. In the United States modafinil is classified as a schedule IV controlled substance and restricted in availability and usage, due to concerns about possible addiction potential. In most other countries it is a prescription drug but not otherwise legally restricted.
Contents
- Medical
- Off label use for fatigue
- Military and astronauts
- Contraindications
- Adverse effects
- Addiction and dependence potential
- Tolerance
- Overdose
- Interactions
- Dopamine transporter blocker
- DAT independent actions
- D2 receptor partial agonist
- Miscellaneous
- Pharmacokinetics
- Measurement in body fluids
- History
- Patent protection and antitrust litigation
- United States
- China
- Japan
- Russia
- Other countries
- Brand names
- Sports
- Nootropic
- ADHD
- Depersonalization disorder
- Psychiatricneurodegenerative disorders
- Cocaine addiction
- Weight loss
- Delayed sleep phase syndrome
- Cognitive enhancement
- Post chemotherapy cognitive impairment
- Motion sickness
- Modafinil analogs
- References
Although the mechanism of action of modafinil was initially unknown, it now appears that the drug acts as a selective, relatively weak, atypical dopamine reuptake inhibitor. However, it appears that other additional mechanisms may also be at play.
Medical
Modafinil is a wakefulness-promoting agent (or eugeroic) used for treatment of narcolepsy, shift work sleep disorder, and excessive daytime sleepiness associated with obstructive sleep apnea.
Because of the risk for development of skin or hypersensitivity reactions and serious adverse psychiatric reactions, the European Medicines Agency has recommended that new patient prescriptions should only be to treat sleepiness associated with narcolepsy.
Off-label use for fatigue
Modafinil has also found off-label use with the neurological fatigue reported by some with multiple sclerosis. In 2000, Cephalon conducted a study to evaluate modafinil as a potential treatment for MS-related fatigue. A group of 72 people with MS of varying degrees of severity tested two different doses of modafinil and an inactive placebo over nine weeks. Fatigue levels were self-evaluated on standardized scales. Participants taking a lower dose of modafinil reported feeling less fatigued and there was a statistically significant difference in fatigue scores for the lower dose versus the placebo. The higher dose of modafinil was not reported to be significantly more effective.
Modafinil is also used off-label to treat sedation and fatigue in many conditions, including depression, fibromyalgia, chronic fatigue syndrome, myotonic dystrophy, opioid-induced sleepiness, spastic cerebral palsy, and Parkinson's disease. Modafinil has been shown to improve excessive daytime somnolence and fatigue in primary biliary cirrhosis.
Military and astronauts
Militaries of several countries are known to have expressed interest in modafinil as an alternative to amphetamine—the drug traditionally employed in combat situations where troops face sleep deprivation, such as during lengthy missions. The French government indicated that the Foreign Legion used modafinil during certain covert operations. The United Kingdom's Ministry of Defence commissioned research into modafinil from QinetiQ and spent £300,000 on one investigation. In 2011, the Indian Air Force announced that modafinil was included in contingency plans.
In the United States military, modafinil has been approved for use on certain Air Force missions, and it is being investigated for other uses. As of November 2012, modafinil is the only drug approved by the Air Force as a "go pill" for fatigue management. The use of dextroamphetamine (a.k.a., Dexedrine) is no longer approved.
The Canadian Medical Association Journal also reports that modafinil is used by astronauts on long-term missions aboard the International Space Station. Modafinil is "available to crew to optimize performance while fatigued" and helps with the disruptions in circadian rhythms and with the reduced quality of sleep astronauts experience.
Contraindications
Allergy and hypersensitivity are the only contraindications of the drug, but literature distributed by Cephalon advises that it is important to consult a physician before using it, as problems may arise for people who are sensitive to constituents of the tablets, people with cirrhosis (which may impair the metabolism of the drug), and people with various cardiovascular problems.
Adverse effects
According to documentation distributed by Teva Pharmaceuticals, one-third of participants in clinical trials reported experiencing headaches; 11% reported nausea; other negative side-effects such as nervousness, diarrhea, insomnia, anxiety, dizziness, and gastrointestinal problems were reported by less than 10% of participants.
Rare occurrences have been reported of more serious adverse effects, including severe skin rashes and other symptoms that are probably allergy-related. From the date of initial marketing, December 1998, to January 30, 2007, the US Food and Drug Administration received six cases of severe cutaneous adverse reactions associated with modafinil, including erythema multiforme (EM), Stevens–Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and DRESS syndrome, involving adult and pediatric patients. The FDA issued a relevant alert. In the same alert, the FDA also noted that angioedema and multi-organ hypersensitivity reactions have also been reported in postmarketing experiences. In 2007, the FDA ordered Cephalon to modify the Provigil leaflet in bold-face print of several serious and potentially fatal conditions attributed to modafinil use, including TEN, DRESS syndrome, and SJS.
The long term safety and effectiveness of modafinil have not been determined.
Modafinil may have an adverse effect on hormonal contraceptives for up to a month after discontinuation.
Addiction and dependence potential
The addiction and dependence liabilities of modafinil are very low. It shares biochemical mechanisms with addictive stimulant drugs, and some studies have reported it to have similar mood-elevating properties, although to a lesser degree. Monkeys will self-administer modafinil if they have previously been trained to self-administer cocaine. Although modafinil does not produce reinforcing effects in mice at doses that are equivalent to those used therapeutically in humans, it does do so at higher doses. In accordance, although very rare, case reports of modafinil abuse exist. As such, modafinil is classified by the United States FDA as a schedule IV controlled substance, a category for drugs with valid medical uses and low but significant addiction potential.
Psychological dependence upon modafinil has only been noted in case reports involving daily overdoses on modafinil for an extended period of time. Reported withdrawal symptoms include anhedonia, lethargy, anxiety, and insomnia.
Tolerance
Large-scale clinical studies have found no evidence of tolerance with modafinil at therapeutic dosages even with prolonged use (for 40 weeks and as long as three years).
Overdose
In mice and rats, the median lethal dose (LD50) of modafinil is approximately or slightly greater than 1250 mg/kg. Oral LD50 values reported for rats range from 1000–3400 mg/kg. Intravenous LD50 for dogs is 300 mg/kg. Clinical trials on humans involving taking up to 1200 mg/day for 7–21 days and known incidents of acute one-time overdoses up to 4500 mg did not appear to cause life-threatening effects, although a number of adverse experiences were observed, including excitation or agitation, insomnia, anxiety, irritability, aggressiveness, confusion, nervousness, tremor, palpitations, sleep disturbances, nausea, and diarrhea. As of 2004, the FDA is not aware of any fatal overdoses involving modafinil alone (as opposed to multiple drugs, including modafinil).
Interactions
Coadministration with modafinil alongside opioids such as hydrocodone, oxycodone, and fentanyl, as well as various other drugs, may experience a drop in plasma concentrations. The reasoning behind this action is because modafinil is an inducer of the CYP3A4 enzymes. If not monitored closely, reduced efficacy or withdrawal symptoms can occur.
Dopamine transporter blocker
Initially, the mechanism of action of modafinil was unknown. Research found that modafinil elevates histamine levels in the hypothalamus in animals. The locus of the monoamine action of modafinil was also the target of studies, with effects identified on dopamine in the striatum and, in particular, nucleus accumbens, norepinephrine in the hypothalamus and ventrolateral preoptic nucleus, and serotonin in the amygdala and frontal cortex. Modafinil was screened at a large panel of receptors and transporters in an attempt to elucidate its pharmacology. Of the sites tested, it was found to significantly affect only on the dopamine transporter (DAT), acting as a dopamine reuptake inhibitor (DRI) with an IC50 value of 4 μM. Subsequently, it was determined that modafinil binds to the same site on the DAT as cocaine, but in a different manner. In accordance, modafinil increases locomotor activity and extracellular dopamine concentrations in animals in a manner similar to the selective DRI vanoxerine (GBR-12909), and also inhibits methamphetamine-induced dopamine release (a common property of DRIs, since DAT transport facilitates methamphetamine's access to its intracellular targets). As such, "modafinil is an exceptionally weak, but apparently very selective, [DAT] inhibitor". In addition to animal research, a human positron emission tomography (PET) imaging study found that 200 mg and 300 mg doses of modafinil resulted in DAT occupancy of 51.4% and 56.9%, respectively, which was described as "close to that of methylphenidate". Another human PET imaging study similarly found that modafinil occupied the DAT and also determined that it significantly elevated extracellular levels of dopamine in the brain, including in the nucleus accumbens.
Modafinil has been described as an "atypical" DAT inhibitor, and shows a profile of effects that is very different from those of other dopaminergic stimulants. For instance, modafinil produces wakefulness reportedly without the need for compensatory sleep, and shows a relatively low, if any, potential for abuse. Aside from modafinil, examples of other atypical DAT inhibitors include vanoxerine and benztropine, which have a relatively low abuse potential similarly to modafinil. These drugs appear to interact molecularly with the DAT in a distinct way relative to "conventional" DAT blockers such as cocaine and methylphenidate.
DAT-independent actions
Against the hypothesis that modafinil exerts its effects by acting as a DRI, tyrosine hydroxylase inhibitors (which deplete dopamine) fail to block the effects of modafinil in animals. In addition, modafinil fails to reverse reserpine-induced akinesia, whereas dextroamphetamine, a dopamine releasing agent (DRA), is able to do so. Moreover, one of the first published structure-activity relationship studies of modafinil found in 2012 that DAT inhibition did not correlate with wakefulness-promoting effects in animals among modafinil analogues, and a variety of analogues without any significant inhibition of the DAT still produced wakefulness-promoting effects. Furthermore, "[the] neurochemical effects [of modafinil] and anatomical pattern of brain area activation differ from typical psychostimulants and are consistent with its beneficial effects on cognitive performance processes such as attention, learning, and memory", and a study found that modafinil-induced increases locomotor activity in animals were dependent on histamine release and could be abolished by depletion of neuronal histamine, whereas those of methylphenidate were not and could not be. As such, although it is established that modafinil is a clinically significant DRI, its full pharmacology remains unclear and may be more complex than this single property (i.e., may also include DAT-independent actions, such as "activation of the orexin system").
In any case, there is nonetheless a good deal of evidence to indicate that modafinil is producing at least a portion of its wakefulness-promoting effects by acting as a DRI, or at least via activation of the dopaminergic system. In support of modafinil acting as a dopaminergic agent, its wakefulness-promoting effects are abolished in DAT knockout mice (although it is important to note that DAT knockout mice show D1 and D2 receptor and norepinephrine compensatory abnormalities, which might confound this finding), reduced by both D1 and D2 receptor antagonists (although conflicting reports exist), and completely blocked by simultaneous inactivation of both D1 and D2 receptors. In accordance, modafinil shows full stimulus generalization to other DAT inhibitors including cocaine, methylphenidate, and vanoxerine, and discrimination is blocked by administration of both ecopipam (SCH-39166), a D1 receptor antagonist, and haloperidol, a D2 receptor antagonist. Partial substitution was seen with the DRA dextroamphetamine and the D2 receptor agonist PNU-91356A, as well as with nicotine (which indirectly elevates dopamine levels through activation of nicotinic acetylcholine receptors).
Modafinil may possess yet an additional mechanism of action. Both modafinil and its metabolite, modafinil sulfone, possess anticonvulsant properties in animals, and modafinil sulfone is nearly as potent as modafinil in producing this effect. However, modafinil sulfone lacks any wakefulness-promoting effects in animals, indicating that a distinct mechanism may be at play in the anticonvulsant effects of both compounds.
D2 receptor partial agonist
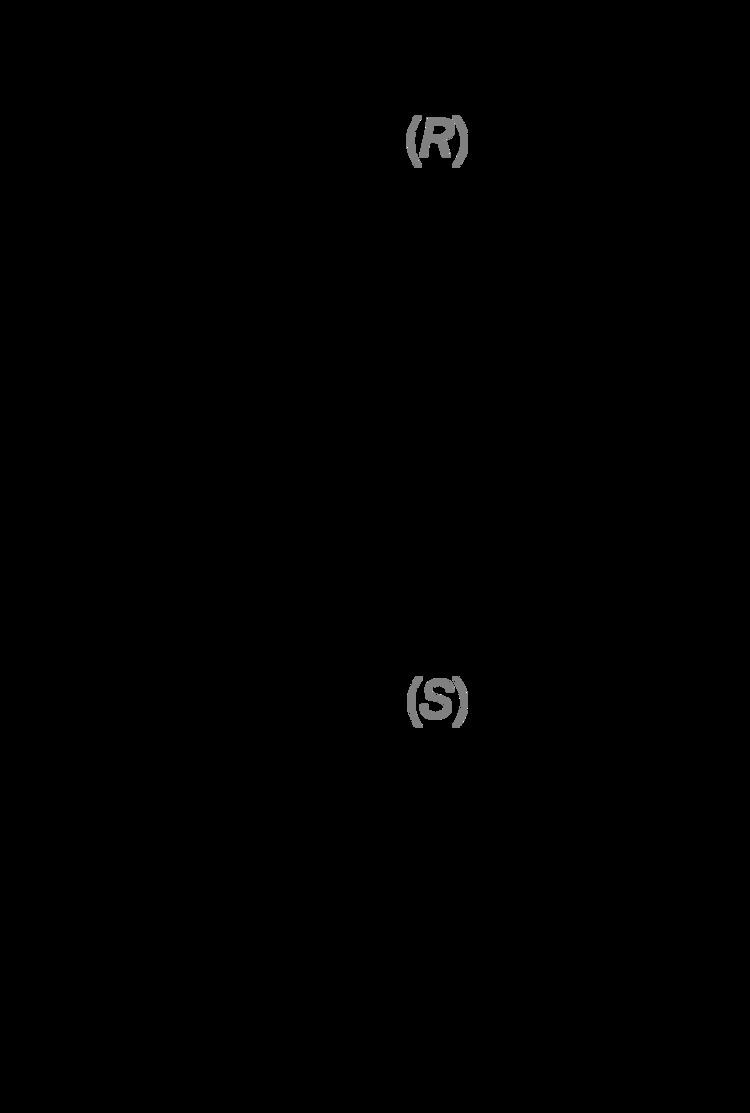
The (R)-(−)-enantiomer of modafinil, known as armodafinil, was also subsequently found to act as a D2High receptor partial agonist, with a Ki of 16 nM, an intrinsic activity of 48%, and an EC50 of 120 nM, in rat striatal tissue. The (S)-enantiomer is inactive with respect to the D2 receptor. Modafinil has been found to directly inhibit the firing of midbrain dopaminergic neurons in the ventral tegmental area and substantia nigra of rats via activation of D2 receptors.
Miscellaneous
Modafinil's efficacy in improving vigor and well-being in sleep deprivation subjects is dependent on catechol-O-methyl transferase (COMT) status. Research suggests that individuals with the Val/Val genotype experience a great improvement in their cognitive function, while those with the Met/Met allele experience very little improvement.
Pharmacokinetics
Modafinil induces the cytochrome P450 enzymes CYP1A2, CYP3A4, and CYP2B6, as well as inhibiting CYP2C9 and CYP2C19 in vitro. It may also induce P-glycoprotein (Pgp), which may affect drugs transported by Pgp, such as digoxin. The bioavailability of modafinil is greater than 80% of the administered dose. In vitro measurements indicate that 60% of modafinil is bound to plasma proteins at clinical concentrations of the drug. This percentage actually changes very little when the concentration is varied. Cmax (peak levels) occurs approximately 2–3 hours after administration. Food slows absorption, but does not affect the total AUC(AUC – area under the curve – meaning, food may slow absorption, but the total amount of the chemical will be absorbed with or without food). Half-life is generally in the 10–12 hour range, subject to differences in CYP genotypes, liver function and renal function. It is metabolized in the liver, and its inactive metabolite is excreted in the urine. Urinary excretion of the unchanged drug ranges from 0% to as high as 18.7%, depending on various factors.
The two major circulating metabolites of modafinil are modafinil acid (CRL-40467) and modafinil sulfone (CRL-41056). Both of these metabolites have been described as inactive, and neither appear to contribute to the wakefulness-promoting effects of modafinil. However, modafinil sulfone does appear to possess anticonvulsant effects, and this is a property that it shares with modafinil.
Measurement in body fluids
Modafinil and/or its major metabolite, modafinil acid, may be quantified in plasma, serum or urine to monitor dosage in those receiving the drug therapeutically, to confirm a diagnosis of poisoning in hospitalized patients or to assist in the forensic investigation of a vehicular traffic violation. Instrumental techniques involving gas or liquid chromatography are usually employed for these purposes. As of 2011, it is not specifically tested for by common drug screens (except for anti-doping screens) and is unlikely to cause false positives for other chemically-unrelated drugs such as substituted amphetamines.
Reagent testing can be used to screen for the presence of modafinil in samples.
History
Modafinil was originally developed in France by neurophysiologist and emeritus experimental medicine professor Michel Jouvet and Lafon Laboratories. Modafinil originated with the late 1970s invention of a series of benzhydryl sulfinyl compounds, including adrafinil, which was first offered as an experimental treatment for narcolepsy in France in 1986. Modafinil is the primary metabolite of adrafinil, lacking the polar -OH group on its terminal amide, and has similar activity to the parent drug but is much more widely used. It has been prescribed in France since 1994 under the name Modiodal, and in the US since 1998 as Provigil.
In 1998, modafinil was approved by the U.S. Food and Drug Administration for the treatment of narcolepsy and in 2003 for shift work sleep disorder and obstructive sleep apnea/hypopnea even though caffeine and amphetamine were shown to be more wakefulness promoting on the Stanford Sleepiness Test Score than modafinil.
It was approved for use in the UK in December 2002. Modafinil is marketed in the US by Cephalon Inc., who originally leased the rights from Lafon, but eventually purchased the company in 2001.
Cephalon began to market the R-enantiomer armodafinil of modafinil in the U.S. in 2007. After protracted patent litigation and negotiations (see below), generic versions of modafinil became available in the U.S. in 2012.
Patent protection and antitrust litigation
U.S. Patent 4,927,855 was issued to Laboratoire L. Lafon on May 22, 1990, covering the chemical compound modafinil. After receiving an interim term extension of 1066 days and pediatric exclusivity of six months, it expired on October 22, 2010. On October 6, 1994, Cephalon filed an additional patent, covering modafinil in the form of particles of defined size. That patent, U.S. Patent 5,618,845 was issued on April 8, 1997, but was reissued in 2002 as RE 37,516, which surrendered the 5618845 patent. With pediatric exclusivity, this patent expired on April 6, 2015.
On December 24, 2002, anticipating the expiration of exclusive marketing rights, generic drug manufacturers Mylan, Teva, Barr, and Ranbaxy applied to the FDA to market a generic form of modafinil. At least one withdrew its application after early opposition by Cephalon based on the '516 patent. There is some question whether a particle size patent is sufficient protection against the manufacture of generics. Pertinent questions include whether modafinil may be modified or manufactured to avoid the granularities specified in the new Cephalon patent, and whether patenting particle size is invalid because particles of appropriate sizes are likely to be obvious to practitioners skilled in the art. However, under United States patent law, a patent is entitled to a legal presumption of validity, meaning that in order to invalidate the patent, much more than "pertinent questions" are required.
As of October 31, 2011, U.S. Reissue Patent No. RE 37,516 has been declared invalid and unenforceable. The District Court for the Eastern District of Pennsylvania ruled that RE 37,516 was invalid because it: (1) was on sale more than one year prior to the date of the application in violation of 35 U.S.C. section 102(b); (2) was actually invented by someone else (the French company Laboratoire L. Lafon); (3) was obvious at the time the invention was made to a person having ordinary skill in the art under 35 U.S.C. section 103(a); and (4) failed the written description requirement of 35 U.S.C. section 112. The patent was also found to be unenforceable due to Cephalon's inequitable conduct during patent prosecution.
Cephalon made an agreement with four major generics manufacturers Teva, Barr Pharmaceuticals, Ranbaxy Laboratories, and Watson Pharmaceuticals between 2005 and 2006 to delay sales of generic modafinil in the US until April 2012 by these companies in exchange for upfront and royalty payments. Litigation arising from these agreements is still pending including an FTC suit filed in April 2008. Apotex received regulatory approval in Canada despite a suit from Cephalon's marketing partner in Canada, Shire Pharmaceuticals. Cephalon has sued Apotex in the US to prevent it from releasing a genericized armodafinil (Nuvigil). Cephalon's 2011 attempt to merge with Teva was approved by the FTC under a number of conditions, including granting generic US rights to another company; ultimately, Par Pharmaceutical acquired the US modafinil rights as well as some others.
In the United Kingdom, Mylan Inc. received regulatory approval to sell generic modafinil produced by Orchid in January 2010; Cephalon sued to prevent sale, but lost the patent trial in November.
United States
Modafinil is currently classified as a Schedule IV controlled substance under United States federal law; it is illegal to import by anyone other than a DEA-registered importer without a prescription. However, one may legally bring modafinil into the United States in person from a foreign country, provided that he or she has a prescription for it, and the drug is properly declared at the border crossing. U.S. residents are limited to 50 dosage units (e.g., pills). Under the US Food and Drug Act, drug companies are not allowed to market their drugs for off-label uses (conditions other than those officially approved by the FDA); Cephalon was reprimanded in 2002 by the FDA because its promotional materials were found to be "false, lacking in fair balance, or otherwise misleading". Cephalon pleaded guilty to a criminal violation and paid several fines, including $50 million and $425 million fines to the U.S. government in 2008.
China
In mainland China, modafinil is strictly controlled like other stimulants, such as amphetamines and methylphenidate, and not approved for medical use.
Japan
In Japan, modafinil is Schedule I psychotropic drug. There have been reported arrests of people who imported modafinil for personal use.
Russia
In Russia modafinil is Schedule II controlled substance like cocaine and morphine. Possession of few modafinil pills can lead to 3—10 years imprisonment.
Other countries
The following countries do not classify modafinil as a controlled substance:
Brand names
Modafinil is sold under a wide variety of brand names worldwide, including Alertec, Alertex, Altasomil, Aspendos, Forcilin, Intensit, Mentix, Modafinil, Modafinilo, Modanil, Modasomil, Modavigil, Modiodal, Modiwake, Movigil, Provigil, Resotyl, Stavigile, Vigia, Vigicer, Vigil, Vigimax, and Zalux.
Sports
The regulation of modafinil as a doping agent has been controversial in the sporting world, with high-profile cases attracting press coverage since several prominent American athletes have tested positive for the substance. Some athletes who were found to have used modafinil protested that the drug was not on the prohibited list at the time of their offenses. However, the World Anti-Doping Agency (WADA) maintains that it was related to already banned substances. The Agency added modafinil to its list of prohibited substances on August 3, 2004, ten days before the start of the 2004 Summer Olympics.
Modafinil has received some publicity in the past when several athletes (such as sprinter Kelli White in 2004, cyclist David Clinger and basketball player Diana Taurasi in 2010, and rower Timothy Grant in 2015) were discovered allegedly using it as a performance-enhancing doping agent. (Taurasi and another player, Monique Coker, tested at the same lab, were later cleared.) It is not clear how widespread this practice is. The BALCO scandal brought to light an as-yet unsubstantiated (but widely published) account of Major League Baseball's all-time leading home-run hitter Barry Bonds' supplemental chemical regimen that included modafinil in addition to anabolic steroids and human growth hormone. Modafinil has been shown to prolong exercise time to exhaustion while performing at 85% of VO2max and also reduces the perception of effort required to maintain this threshold. Modafinil was added to the World Anti-Doping Agency "Prohibited List" in 2004 as a prohibited stimulant (see Modafinil Legal Status).
Nootropic
Modafinil has been used non-medically as a "smart drug" by students and office workers.
ADHD
Double-blind randomized controlled trials have demonstrated the efficacy and tolerability of modafinil in pediatric ADHD, however there are risks of serious side effects such as skin reactions and modafinil is not recommended for use in children. In the United States, it was originally pending marketing as Sparlon for pediatric ADHD, but approval was denied by the FDA due to major concerns over the occurrence of Stevens-Johnson Syndrome in clinical trials.
Depersonalization disorder
Modafinil used alone has been reported to be effective in a subgroup of individuals with depersonalization disorder; the subgroup of people with depersonalization disorder most likely to respond are those who have attentional impairments, under-arousal, and hypersomnia. However, clinical trials have not been conducted. Dr. Evan Torch calls a combination of an SSRI and modafinil "the hidden pearl that can really help depersonalization disorder."
Psychiatric/neurodegenerative disorders
It has been studied for depression, bipolar depression, opiate and cocaine dependence, Parkinson's disease, schizophrenia, and disease-related fatigue, as well as fatigue that is the side effect of another medication.
Modafinil may also be an effective and well-tolerated treatment in patients with seasonal affective disorder.
A randomized double-blind study of modafinil showed that normal healthy volunteers between the ages of 30–44 showed general improvement in alertness as well as mood. In the three-day study, counterbalanced, randomized, crossover, inpatient trial of modafinil 400 mg was administered as well as a placebo to the control group. The conclusion demonstrated that modafinil may have general mood-elevating effects in particular for the adjunctive use in treatment-resistant depression.
Cocaine addiction
Modafinil is under investigation as a possible method to treat cocaine dependence, for several reasons involving biochemical mechanisms of the two drugs, as well as the observation that clinical effects of modafinil are largely opposite to symptoms of cocaine withdrawal.
The pilot 8-week double-blind study of modafinil for cocaine dependence (2004) produced inconclusive results. The number of cocaine-positive urine samples was significantly lower in the modafinil group as compared to the placebo group in the middle of the trial, but by the end of the 8 weeks the difference stopped being significant. Even before the treatment began, the modafinil group had lower cocaine consumption further confounding the results. As compared to placebo, modafinil did not reduce cocaine craving or self-reported cocaine use, and the physicians ratings were only insignificantly better. Dan Umanoff, of the National Association for the Advancement and Advocacy of Addicts, criticized the authors of the study for leaving the negative results out of the discussion part and the abstract of the article.
A later double-blind study of modafinil in people seeking treatment for cocaine dependence found no statistically significant effect on the rate of change in percentage of cocaine non-use days, but noted a significant improvement in some secondary outcomes such as the maximum number of consecutive non-use days for cocaine.
Weight loss
Studies on modafinil (even those on healthy weight individuals) indicate that it has an appetite reducing/weight loss effect. All studies on modafinil in the Medline database that are for one month or longer which report weight changes find that modafinil users experience weight loss compared to placebo. In 2008, one small-scale study on individuals performing simulated shift work quantified the effect as an 18% decrease in total caloric intake on 200 mg/day, and a 38% decrease on 400 mg/day.
However, the prescribing information for Provigil notes that "There were no clinically significant differences in body weight change in patients treated with Provigil compared to placebo-treated patients in the placebo-controlled clinical trials."
In experimental studies, the appetite reducing effect of modafinil appears to be similar to that of substituted amphetamines, but, unlike substituted amphetamines, the dose of modafinil that is effective at decreasing food intake does not significantly increase heart rate. Also, an article published in the Annals of Clinical Psychiatry, presented the case of a 280-pound patient (BMI=35.52) who lost 40 pounds over the course of a year on modafinil (to 30.44 BMI). After three years, his weight stabilized at a 50-pound weight loss (29.59 BMI). The authors conclude that placebo controlled studies should be conducted on using modafinil as a weight loss agent. Conversely, a US patent (#6,455,588) on using modafinil as an appetite stimulating agent has been filed by Cephalon in 2000.
Delayed sleep phase syndrome
Modafinil has been studied as a possible treatment for delayed sleep phase syndrome, which causes excessive daytime somnolence when the natural (delayed) diurnal rhythm is replaced by a socially determined earlier or forward shifted sleep schedule.
Cognitive enhancement
There is disagreement to whether the cognitive effects modafinil showed in healthy non-sleep-deprived people are sufficient to consider it to be a cognitive enhancer. The researchers agree that modafinil improves some aspects of working memory, such as digit span, digit manipulation and pattern recognition memory, but the results related to spatial memory, executive function and attention are equivocal. Some positive effects of modafinil may be limited to "lower-performing" individuals. One study found that modafinil restored normal levels of learning ability in methamphetamine addicts, but had no effect on non-addicts. Modafinil reduces the symptoms of attention-deficit hyperactivity disorder and improves working and episodic memory.
Post-chemotherapy cognitive impairment
Modafinil has been used off-label in trials with people with symptoms of post-chemotherapy cognitive impairment, also known as "chemobrain", but in 2011 it was found to be no better than placebo. As of 2015 it had been studied for use in multiple sclerosis associated fatigue, but the resulting evidence was weak and inconclusive.
Motion sickness
Modafinil has been evaluated alone and in combination with scopolamine as an anti-motion sickness medication. It did not help by itself, but appeared to help in combination with scopolamine, acting to reduce symptoms of drowsiness associated with scopolamine.
Modafinil analogs
Modafinil is a highly researched compound, with many derivatives created and studied, some examples and their differences between dopamine, serotonin & norepinephrine affect is given in bundled table form below.