
ICD-9-CM 281 MedlinePlus 000567 | ICD-10 D51.1, D52.0, D53.1 DiseasesDB 29507 eMedicine med/1420 ped/2575 | |
 | ||
Megaloblastic anemia (or megaloblastic anaemia) is an anemia (of macrocytic classification) that results from inhibition of DNA synthesis during red blood cell production. When DNA synthesis is impaired, the cell cycle cannot progress from the G2 growth stage to the mitosis (M) stage. This leads to continuing cell growth without division, which presents as macrocytosis. Megaloblastic anemia has a rather slow onset, especially when compared to that of other anemias. The defect in red cell DNA synthesis is most often due to hypovitaminosis, specifically a deficiency of vitamin B and/or folic acid. Vitamin B deficiency alone will not cause the syndrome in the presence of sufficient folate, as the mechanism is loss of B dependent folate recycling, followed by folate-deficiency loss of nucleic acid synthesis (specifically thymine), leading to defects in DNA synthesis. Folic acid supplementation in the absence of vitamin B prevents this type of anemia (although other vitamin B-specific pathologies may be present). Loss of micronutrients may also be a cause. Copper deficiency resulting from an excess of zinc from unusually high oral consumption of zinc-containing denture-fixation creams has been found to be a cause.
Contents
Megaloblastic anemia not due to hypovitaminosis may be caused by antimetabolites that poison DNA production directly, such as some chemotherapeutic or antimicrobial agents (for example azathioprine or trimethoprim).
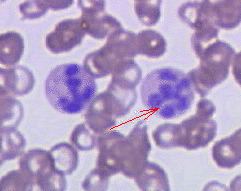
The pathological state of megaloblastosis is characterized by many large immature and dysfunctional red blood cells (megaloblasts) in the bone marrow and also by hypersegmented neutrophils (those exhibiting five or more nuclear lobes ("segments"), with up to four lobes being normal). These hypersegmented neutrophils are found in the "peripheral blood" (i.e., a diagnostic smear of a blood-sample taken from the circulation).
Causes
Hematological findings
The blood film can point towards vitamin deficiency:
Blood chemistries will also show:
Normal levels of both methylmalonic acid and total homocysteine rule out clinically significant cobalamin deficiency with virtual certainty.
Bone marrow (not normally checked in a patient suspected of megaloblastic anemia) shows megaloblastic hyperplasia.
Analysis
The gold standard for the diagnosis of Vitamin B12 deficiency is a low blood level of Vitamin B12. A low level of blood Vitamin B12 is a finding that normally can and should be treated by injections, supplementation, or dietary or lifestyle advice, but it is not a diagnosis. Hypovitaminosis B12 can result from a number of mechanisms, including those listed above. For determination of etiology, further patient history, testing, and empirical therapy may be clinically indicated.
A measurement of methylmalonic acid (methylmalonate) can provide an indirect method for partially differentiating Vitamin B12 and folate deficiencies. The level of methylmalonic acid is not elevated in folic acid deficiency. Direct measurement of blood cobalamin remains the gold standard because the test for elevated methylmalonic acid is not specific enough. Vitamin B12 is one necessary prosthetic group to the enzyme methylmalonyl-coenzyme A mutase. Vitamin B12 deficiency is but one among the conditions that can lead to dysfunction of this enzyme and a buildup of its substrate, methylmalonic acid, the elevated level of which can be detected in the urine and blood.
Due to the lack of available radioactive Vitamin B12, the Schilling test is now largely a historical artifact. The Schilling test was performed in the past to help determine the nature of the vitamin B12 deficiency. An advantage of the Schilling test was that it often included Vitamin B12 with intrinsic factor.