
ICD-9-CM 562.00 DiseasesDB 3871 | ICD-10 K57 OMIM 223320 eMedicine med/3102 | |
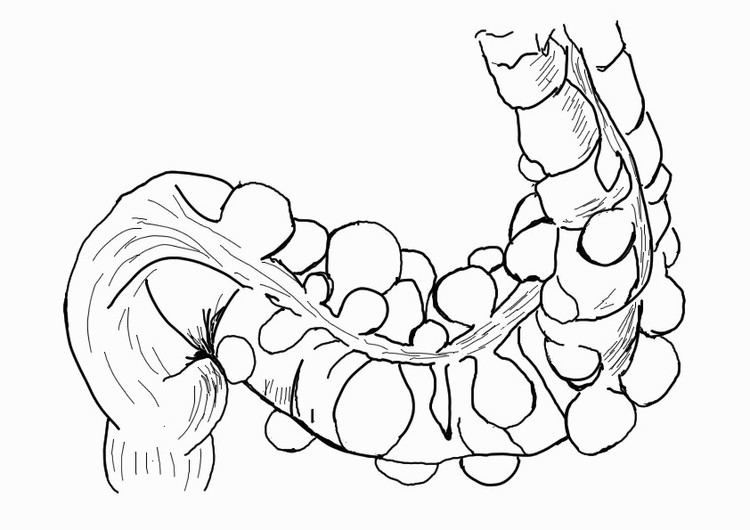 | ||
Diverticulosis is the condition of having diverticula in the colon that are not inflamed. These are outpockets of the colonic mucosa and submucosa through weaknesses of muscle layers in the colon wall. They typically cause no symptoms. Diverticular disease occurs when diverticula become inflamed, known as diverticulitis, or bleed.
Contents
- Signs and symptoms
- Bleeding
- Diverticulitis
- Risk factors
- Diagnosis
- Management
- Diet
- Complications
- Epidemiology
- Economics
- References
They typically occur in the sigmoid colon, which is a common place for increased pressure. The left side is more commonly affected in the United States while the right side is more commonly affected in Asia. Diagnosis is often during routine colonoscopy or as an incidental finding during CT scan.
It is common in Western countries with about half of those over the age of 60 in Canada and the United States affected. Diverticula are uncommon before the age of 40, and increase in incidence beyond that age. Rates are lower in Africa which has been attributed to a shorter life expectancy and poor healthcare access. The lower rate has also been attributed to high fiber.
Signs and symptoms
Some people with diverticulosis complain of symptoms such as cramping, bloating, flatulence, and irregular defecation. However, it is unclear if these symptoms are attributable to the underlying diverticulosis or to coexistent irritable bowel syndrome.
Diverticular disease was found associated with a higher risk of left sided colon cancer.
Bleeding
Diverticular disease can present with painless rectal bleeding as bright red blood per rectum. Diverticular bleeding is the most common cause of acute lower gastrointestinal bleeding. However, it is estimated that 80% of these cases are self-limiting and require no specific therapy.
Diverticulitis
Infection of a diverticulum can result in diverticulitis. This occurs in 10–25% of people with diverticulosis. Tears in the colon leading to bleeding or perforations may occur; intestinal obstruction may occur (constipation or diarrhea does not rule this possibility out); and peritonitis, abscess formation, retroperitoneal fibrosis, sepsis, and fistula formation are also possible occurrences. Rarely, an enterolith may form. Infection of a diverticulum often occurs as a result of stool collecting in a diverticulum.
It is defined as diverticular disease with signs and symptoms of diverticular inflammation. Clinical features of acute diverticulitis include constant abdominal pain, localized abdominal tenderness in the left lower quadrant of the abdomen, nausea, vomiting, constipation or diarrhea, fever and leucocytosis.
Most people with colonic diverticulosis are unaware of this structural change. When symptoms do appear in a person over 40 years of age it is important to obtain medical advice and exclude more dangerous conditions such as cancer of the colon or rectum.
Risk factors
- increasing age
- constipation
- a diet that is low in dietary fiber (although this claim is controversial)
- connective tissue disorders (such as Marfan syndrome and Ehlers Danlos Syndrome) that may cause weakness in the colon wall
- hereditary or genetic predisposition,
- extreme weight loss
- heavy meat consumption
The exact etiology of colonic diverticulosis has yet to be fully clarified and many of the claims are only anecdotal. The modern emphasis on the value of fiber in the diet began with Cleave. A strong case was made by Neil Painter and Adam Smith that a deficiency of dietary fiber is the cause of diverticular disease. They argued that the colonic muscles needed to contract strongly in order to transmit and expel the small stool associated with a fiber deficient diet. The increased pressure within the segmented section of bowel over years gave rise to herniation at the vulnerable point where blood vessels enter the colonic wall.
The U.S. National Institutes of Health (NIH) notes that, although the low-fiber theory of the cause of diverticulosis is the leading theory, it has not yet been proven. Furthermore, a February 2012 study of 2,104 male participants found that "A high-fiber diet and increased frequency of bowel movements are associated with greater, rather than lower, prevalence of diverticulosis."
Denis Burkitt suggested that the mechanical properties of the colon may be different in the African and the European subjects. He theorized that because Africans eat a diet containing more fiber than Europeans and use the natural squatting position for defecation, they pass bulky stools without straining, and hence rarely if ever develop colonic diverticulosis.
Change in the strength of the colonic wall with age may be a cause. Connective tissue is a significant contributor to the strength of the colonic wall. The mechanical properties of connective tissue depend on a wide variety of factors, the type of tissue and its age, the nature of the intramolecular and intermolecular covalent cross links and the quantity of the glycosaminoglycans associated with the collagen fibrils. The submucosa of the colon is composed almost entirely of collagen, both type I and type III. Several layers of collagen fibres make up the submucosa of the human colon. The collagen fibril diameters and fibril counts are different between the left and right colon and change with age and in colonic diverticulosis,. The implication is that changes normally associated with ageing are more pronounced in colonic diverticulosis. Iwasaki found that the tensile strength of the Japanese colon obtained at postmortem declined with age. Similarly the mechanical properties of the colon are stronger in African than European subjects. However, this race-based claim is contradicted by the virtually identical incidence of diverticular disease in black and white Americans.
The strength of the colon decreases with age in all parts of the colon, except the ascending colon. The fall in tensile strength with age is due to a decrease in the integrity of connective tissue. Cross linkage of collagen is increased in colonic diverticulosis. The mucosal layer is possibly more elastic and it is likely that the stiffer external layers break and allow the elastic mucosa to herniate through forming a diverticulum. Collagen has intermolecular and intramolecular cross links which stabilise and give strength to the tissue in which it is located. Accumulation of covalently linked sugar molecules and related increasing cross linking products are found in a variety of tissues with ageing, skin, vascular tissue, the cordae tendinae of heart valves and the colon. This reduces the strength and pliability of the collagen. Colonic diverticulosis increases in frequency with age. There is a reduction in the strength of the colonic mucosa with age, and that increased contractions in the descending and sigmoid colon secondary to an insufficient fibre content of the diet cause protrusion through this weakened wall. Colonic diverticulosis is in general a benign condition of the bowel which uncommonly becomes symptomatic and even less commonly becomes a truly clinical complicated problem.
Diagnosis
In cases of asymptomatic diverticulosis, the diagnosis is usually made as an incidental finding on other investigations.
While a good history is often sufficient to form a diagnosis of diverticulosis or diverticulitis, it is important to confirm the diagnosis and rule out other pathology (notably colorectal cancer) and complications.
Investigations
It is important to note that both barium enema and colonoscopy are contraindicated during acute episodes of diverticulitis, as the barium may leak out into the abdominal cavity, and colonoscopy can cause perforations of the bowel wall.
Management
Many people with diverticulosis have minimal to no symptoms, and do not require any specific treatment. Colonic stimulants should be avoided. Treatments, like some colon cleansers, that cause hard stools, constipation, and straining, are not recommended.
Diet
A high-fiber diet and fiber supplements are advisable to prevent constipation. The American Dietetic Association recommends 20–35 grams each day. Wheat bran has much to commend it as this has been shown to reduce intra colonic pressure.
The US National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) says foods such as nuts, popcorn hulls, sunflower seeds, pumpkin seeds, caraway seeds, and sesame seeds have traditionally been labeled as problem foods for people with this condition; however, no scientific data exists to prove this hypothesis. The seeds in tomatoes, zucchini, cucumbers, strawberries, raspberries, and poppy seeds, are not considered harmful by the NIDDK.
One study found that nuts and popcorn do not contribute positively or negatively to patients with diverticulosis or diverticular complications.
Complications
Complicated diverticulosis requires treatment of the complication. These complications are often grouped under a single diagnosis of diverticulitis and require skilled medical care of the infection, bleeding and perforation which may include intensive antibiotic treatment, intravenous fluids and surgery. Complications are more common in patients who are taking NSAIDs or aspirin. As diverticulosis occurs in an older population such complications are serious events.
Epidemiology
More than 10% of the U.S. population over the age of 40 and 50% over the age of 60 have diverticulosis. This disease is common in the U.S., Britain, Australia, Canada, and is uncommon in Asia and Africa. Large-mouth diverticula are associated with scleroderma. Diverticular disease is more common in collagen disorders such as Ehlers Danlos Syndrome.
Economics
"The complications of diverticulosis cause considerable morbidity in the United States; health care expenditures for this disorder are estimated to be $2.5 billion per year."