
MeSH D021061 | ||
 | ||
Liquid breathing interview with thomas shaffer
Liquid breathing is a form of respiration in which a normally air-breathing organism breathes an oxygen-rich liquid (such as a perfluorocarbon), rather than breathing air.
Contents
- Liquid breathing interview with thomas shaffer
- Cute science liquid breathing 3
- Approaches
- Total liquid ventilation
- Partial liquid ventilation
- PFC vapor
- Aerosol PFC
- Diving
- Medical treatment
- Space travel
- Examples in fiction
- References

Perfluorochemical (perfluorocarbon) molecules have very different structures that impart different physical properties such as respiratory gas solubility, density, viscosity, vapor pressure, and lipid solubility. Thus, it is critical to choose the appropriate PFC for a specific biomedical application, such as liquid ventilation, drug delivery or blood substitutes. The physical properties of PFC liquids vary substantially; however, the one common property is their high solubility for respiratory gases. In fact, these liquids carry more oxygen and carbon dioxide than blood.

In theory, liquid breathing could assist in the treatment of patients with severe pulmonary or cardiac trauma, especially in pediatric cases. Liquid breathing has also been proposed for use in deep diving and space travel. Despite some recent advances in liquid ventilation, a standard mode of application has not yet been established.
Cute science liquid breathing 3
Approaches
Because liquid breathing is still a highly experimental technique, there are several proposed approaches.
Total liquid ventilation

Although total liquid ventilation (TLV) with completely liquid-filled lungs can be beneficial, the complex liquid-filled tube system required is a disadvantage compared to gas ventilation—the system must incorporate a membrane oxygenator, heater, and pumps to deliver to, and remove from the lungs tidal volume aliquots of conditioned perfluorocarbon (PFC). One research group led by Thomas H. Shaffer has maintained that with the use of microprocessors and new technology, it is possible to maintain better control of respiratory variables such as liquid functional residual capacity and tidal volume during TLV than with gas ventilation. Consequently, the total liquid ventilation necessitates a dedicated liquid ventilator similar to a medical ventilator except that it uses a breatheable liquid. Many prototypes are used for animal experimentation, but experts recommend continued development of a liquid ventilator toward clinical applications. Specific preclinical liquid ventilator (Inolivent) is currently under joint development in Canada and France. The main application of this liquid ventilator is the ultra-fast induction of therapeutic hypothermia after cardiac arrest. This has been demonstrated to be more protective than slower cooling method after experimental cardiac arrest.
Partial liquid ventilation
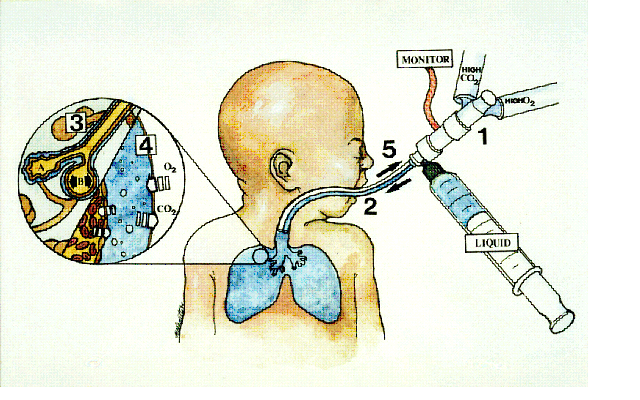
In contrast, partial liquid ventilation (PLV) is a technique in which a PFC is instilled into the lung to a volume approximating functional residual capacity (approximately 40% of total lung capacity). Conventional mechanical ventilation delivers tidal volume breaths on top of it. This mode of liquid ventilation currently seems technologically more feasible than total liquid ventilation, because PLV could utilise technology currently in place in many neonatal intensive-care units (NICU) worldwide.

The influence of PLV on oxygenation, carbon dioxide removal and lung mechanics has been investigated in several animal studies using different models of lung injury. Clinical applications of PLV have been reported in patients with acute respiratory distress syndrome (ARDS), meconium aspiration syndrome, congenital diaphragmatic hernia and respiratory distress syndrome (RDS) of neonates. In order to correctly and effectively conduct PLV, it is essential to
- properly dose a patient to a specific lung volume (10–15 ml/kg) to recruit alveolar volume
- redose the lung with PFC liquid (1–2 ml/kg/h) to oppose PFC evaporation from the lung.
If PFC liquid is not maintained in the lung, PLV can not effectively protect the lung from biophysical forces associated with the gas ventilator.
New application modes for PFC have been developed.
Partial liquid ventilation (PLV) involves filling the lungs with a fluid. This fluid is perfluorocarbon, also called Liquivent or perflubron. The liquid has some unique properties. It has a very low surface tension, similar to surfactant, a substance that is produced in the lungs to prevent the alveoli from collapsing and sticking together during exhalation. It also has a high density, oxygen readily diffuses through it, and it may have some anti-inflammatory properties. In PLV, the lungs are filled with the liquid, the patient is then ventilated with a conventional ventilator using a protective lung ventilation strategy. This is called partial liquid ventilation. The hope is that the liquid will help the transport of oxygen to parts of the lung that are flooded and filled with debris, help remove this debris and open up more alveoli improving lung function. The study of PLV involves comparison to protocolized ventilator strategy designed to minimize lung damage.
PFC vapor
Vaporization of perfluorohexane with two anesthetic vaporizers calibrated for perfluorohexane has been shown to improve gas exchange in oleic acid-induced lung injury in sheep.
Predominantly PFCs with high vapor pressure are suitable for vaporization.
Aerosol-PFC
With aerosolized perfluorooctane, significant improvement of oxygenation and pulmonary mechanics was shown in adult sheep with oleic acid-induced lung injury.
In surfactant-depleted piglets, persistent improvement of gas exchange and lung mechanics was demonstrated with Aerosol-PFC. The aerosol device is of decisive importance for the efficacy of PFC aerosolization, as aerosolization of PF5080 (a less purified FC77) has been shown to be ineffective using a different aerosol device in surfactant-depleted rabbits. Partial liquid ventilation and Aerosol-PFC reduced pulmonary inflammatory response.
Diving
Gas pressure increases with depth, rising 1 bar (14.5 psi (100 kPa)) every 10 meters to over 1,000 bar at the bottom of the Mariana Trench. Diving becomes more dangerous as depth increases, and deep diving presents many hazards. All surface-breathing animals are subject to decompression sickness, including aquatic mammals and free-diving humans (see taravana). Breathing at depth can cause nitrogen narcosis and oxygen toxicity. Holding the breath while ascending after breathing at depth can cause air embolisms, burst lung, and collapsed lung.
Special breathing gas mixes such as trimix or heliox ameliorate the risk of decompression illness but do not eliminate it. Heliox further eliminates the risk of nitrogen narcosis but introduces the risk of helium tremors below 500 feet (152 meters). Atmospheric diving suits maintain body and breathing pressure at 1 bar, eliminating most of the hazards of descending, ascending, and breathing at depth. However, the rigid suits are bulky, clumsy, and very expensive.
Liquid breathing offers a third option, promising the mobility available with flexible dive suits and the reduced risks of rigid suits. With liquid in the lungs, the pressure within the diver's lungs could accommodate changes in the pressure of the surrounding water without the huge gas partial pressure exposures required when the lungs are filled with gas. Liquid breathing would not result in the saturation of body tissues with high pressure nitrogen or helium that occurs with the use of non-liquids, thus would reduce or remove the need for slow decompression.
A significant problem, however, arises from the high viscosity of the liquid and the corresponding reduction in its ability to remove CO2. All uses of liquid breathing for diving must involve total liquid ventilation (see above). Total liquid ventilation, however, has difficulty moving enough liquid to carry away CO2, because no matter how great the total pressure is, the amount of partial CO2 gas pressure available to dissolve CO2 into the breathing liquid can never be much more than the pressure at which CO2 exists in the blood (about 40 mm of mercury (Torr)).
At these pressures, most fluorocarbon liquids require about 70 mL/kg minute-ventilation volumes of liquid (about 5 L/min for a 70 kg adult) to remove enough CO2 for normal resting metabolism. This is a great deal of fluid to move, particularly as liquids are more viscous and denser than gases, (for example water is about 850 times the density of air). Any increase in the diver's metabolic activity also increases CO2 production and the breathing rate, which is already at the limits of realistic flow rates in liquid breathing. It seems unlikely that a person would move 10 liters/min of fluorocarbon liquid without assistance from a mechanical ventilator, so "free breathing" may be unlikely. However, it has been suggested that a liquid breathing system could be combined with a CO2 scrubber connected to the diver's blood supply; a US patent has been filed for such a method.
Medical treatment
The most promising area for the use of liquid ventilation is in the field of pediatric medicine. The first medical use of liquid breathing was treatment of premature babies and adults with acute respiratory distress syndrome (ARDS) in the 1990s. Liquid breathing was used in clinical trials after the development by Alliance Pharmaceuticals of the fluorochemical perfluorooctyl bromide, or perflubron for short. Current methods of positive-pressure ventilation can contribute to the development of lung disease in pre-term neonates, leading to diseases such as bronchopulmonary dysplasia. Liquid ventilation removes many of the high pressure gradients responsible for this damage. Furthermore, perfluorocarbons have been demonstrated to reduce lung inflammation, improve ventilation-perfusion mismatch and to provide a novel route for the pulmonary administration of drugs.
In order to explore drug delivery techniques that would be useful for both partial and total liquid ventilation, more recent studies have focused on PFC drug delivery using a nanocrystal suspension. The first image is a computer model of a PFC liquid (perflubron) combined with gentamicin molecules.
The second image shows experimental results comparing both plasma and tissue levels of gentamicin after an intratracheal (IT) and intravenous (IV) dose of 5 mg/kg in a newborn lamb during gas ventilation. Note that the plasma levels of the IV dose greatly exceed the levels of the IT dose over the 4 hour study period; whereas, the lung tissue levels of gentamicin when delivered by an intratracheal (IT) suspension, uniformly exceed the intravenous (IV) delivery approach after 4 hours. Thus, the IT approach allows more effective delivery of the drug to the target organ while maintaining a safer level systemically. Both images represent the in-vivo time course over 4 hours. Numerous studies have now demonstrated the effectiveness of PFC liquids as a delivery vehicle to the lungs.
Clinical trials with premature infants, children and adults were conducted. Since the safety of the procedure and the effectiveness were apparent from an early stage, the US Food and Drug Administration (FDA) gave the product "fast track" status (meaning an accelerated review of the product, designed to get it to the public as quickly as is safely possible) due to its life-saving potential. Clinical trials showed that using perflubron with ordinary ventilators improved outcomes as much as using high frequency oscillating ventilation (HFOV). But because perflubron was not better than HFOV, the FDA did not approve perflubron, and Alliance is no longer pursuing the partial liquid ventilation application. Whether perflubron would improve outcomes when used with HFOV or has fewer long-term consequences than HFOV remains an open question.
In 1996 Mike Darwin and Steven B. Harris proposed using cold liquid ventilation with perfluorocarbon to quickly lower the body temperature of victims of cardiac arrest and other brain trauma to allow the brain to better recover. The technology came to be called gas/liquid ventilation (GLV), and was shown able to achieve a cooling rate of 0.5 °C per minute in large animals. It has not yet been tried in humans.
Most recently, hypothermic brain protection has been associated with rapid brain cooling. In this regard, a new therapeutic approach is the use of intranasal perfluorochemical spray for preferential brain cooling. The nasopharyngeal (NP) approach is unique for brain cooling due to anatomic proximity to the cerebral circulation and arteries. Based on preclinical studies in adult sheep, it was shown that independent of region, brain cooling was faster during NP-perfluorochemical versus conventional whole body cooling with cooling blankets. To date, there have been four human studies including a completed randomized intra-arrest study (200 patients). Results clearly demonstrated that prehospital intra-arrest transnasal cooling is safe, feasible and is associated with an improvement in cooling time.
Space travel
Liquid immersion provides a way to reduce the physical stress of G forces. Forces applied to fluids are distributed as omnidirectional pressures. Because liquids cannot be practically compressed, they do not change density under high acceleration such as performed in aerial maneuvers or space travel. A person immersed in liquid of the same density as tissue has acceleration forces distributed around the body, rather than applied at a single point such as a seat or harness straps. This principle is used in a new type of G-suit called the Libelle G-suit, which allows aircraft pilots to remain conscious and functioning at more than 10 G acceleration by surrounding them with water in a rigid suit.
Acceleration protection by liquid immersion is limited by the differential density of body tissues and immersion fluid, limiting the utility of this method to about 15 to 20 G. Extending acceleration protection beyond 20 G requires filling the lungs with fluid of density similar to water. An astronaut totally immersed in liquid, with liquid inside all body cavities, will feel little effect from extreme G forces because the forces on a liquid are distributed equally, and in all directions simultaneously. However effects will be felt because of density differences between different body tissues, so an upper acceleration limit still exists.
Liquid breathing for acceleration protection may never be practical because of the difficulty of finding a suitable breathing medium of similar density to water that is compatible with lung tissue. Perfluorocarbon fluids are twice as dense as water, hence unsuitable for this application.