
 | ||
Sodium channel blockers easy pharm for usmle step 1
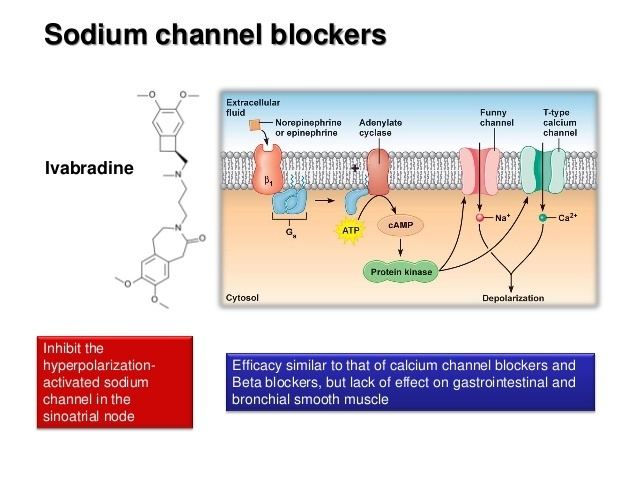
Sodium channel blockers are drugs which impair conduction of sodium ions (Na+) through sodium channels.
Contents
Sodium channel blocker
Extracellular
The following naturally-produced substances block sodium channels by binding to and occluding the extracellular pore opening of the channel:
Intracellular
Drugs which block sodium channels by blocking from the intracellular side of the channel include:
Unknown mechanism
Antiarrhythmic
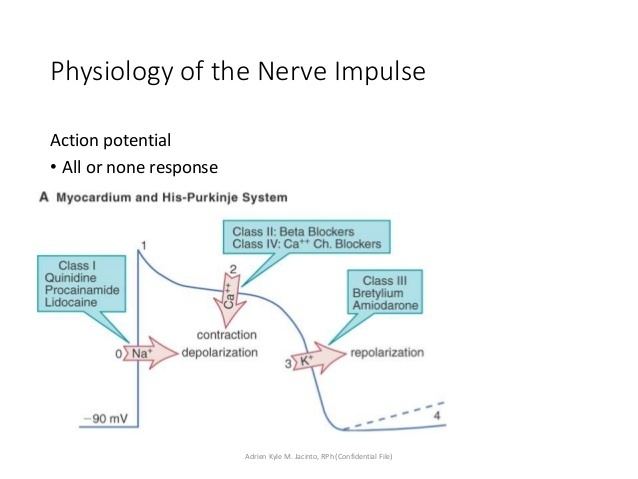
Sodium channel blockers are used in the treatment of cardiac arrhythmia. They are classified as "Type I" in the Vaughan Williams classification.
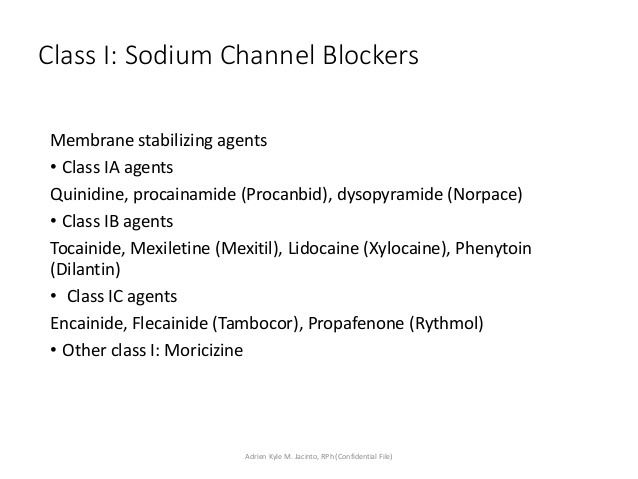
Class I antiarrhythmic agents interfere with the (Na+) channel. Class I agents are grouped by their effect on the Na+ channel, and by their effect on cardiac action potentials. Class I agents are called Membrane Stabilizing Agents. 'Stabilizing' refers to the decrease of excitogenicity of the plasma membrane effected by these agents. A few class II agents, propranolol for example, also have a membrane stabilizing effect.
Class Ia agents
Class Ia agents block the fast sodium channel, which depresses the phase 0 depolarization (i.e. reduces Vmax), which prolongs the action potential duration by slowing conduction. Agents in this class also cause decreased conductivity and increased refractoriness.
Indications for Class Ia agents are supraventricular tachycardia, ventricular tachycardia, symptomatic ventricular premature beats, and prevention of ventricular fibrillation.
Procainamide can be used to treat atrial fibrillation in the setting of Wolff-Parkinson-White syndrome, and to treat wide complex hemodynamically stable tachycardias. Oral procainamide is no longer being manufactured in the US, but intravenous formulations are still available.
While procainamide and quinidine may be used in the conversion of atrial fibrillation to normal sinus rhythm, they should only be used in conjunction with an AV node blocking agent such as digoxin or verapamil, or a beta blocker), because procainamide and quinidine can increase the conduction through the AV node and may cause 1:1 conduction of atrial fibrillation, causing an increase in the ventricular rate.
Class Ia agents include quinidine, procainamide and disopyramide.
Class Ib agents
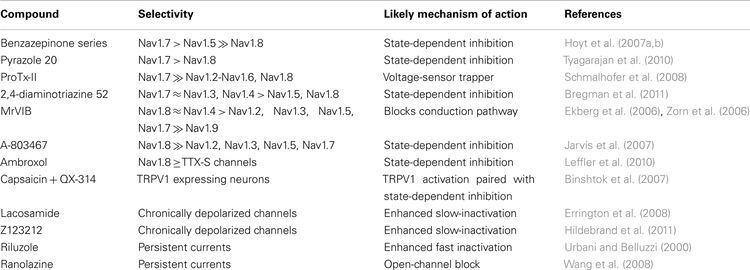
Class Ib antiarrhythmic agents are sodium channel blockers. They have fast onset and offset kinetics, meaning that they have little or no effect at slower heart rates, and more effects at faster heart rates. Class Ib agents shorten the action potential duration and reduce refractoriness. These agents will decrease Vmax in partially depolarized cells with fast response action potentials. They either do not change the action potential duration, or they may decrease the action potential duration. Class Ib drugs tend to be more specific for voltage gated Na channels than Ia. Lidocaine in particular is highly frequency dependent, in that it has more activity with increasing heart rates. This is because lidocaine selectively blocks Na channels in their open and inactive states and has little binding capability in the resting state.
Class Ib agents are indicated for the treatment of ventricular tachycardia and symptomatic premature ventricular beats, and prevention of ventricular fibrillation.
Class Ib agents include lidocaine, mexiletine, tocainide, and phenytoin.
Class Ic agents
Class Ic antiarrhythmic agents markedly depress the phase 0 depolarization (decreasing Vmax). They decrease conductivity, but have a minimal effect on the action potential duration. Of the sodium channel blocking antiarrhythmic agents (the class I antiarrhythmic agents), the class Ic agents have the most potent sodium channel blocking effects.
Class Ic agents are indicated for life-threatening ventricular tachycardia or ventricular fibrillation, and for the treatment of refractory supraventricular tachycardia (i.e. atrial fibrillation). These agents are potentially pro-arrhythmic, especially in settings of structural heart disease (e.g. post-myocardial infarction), and are contraindicated in such settings.
Class Ic agents include encainide, flecainide, moricizine, and propafenone. Encainide is not available in the United States.
Other uses
Sodium channel blockers are also used as local anesthetics and anticonvulsants.
Sodium channel blockers have been proposed for use in the treatment of cystic fibrosis, but current evidence is mixed.
It has been suggested that the analgesic effects of some antidepressants may be mediated in part via sodium channel blockade.
Future prospects
Selective blockers of Nav1.7 and Nav1.8 voltage-gated sodium channels, such as CNV1014802 and Funapide, are being investigated as novel analgesics.