
MeSH D006486 | ||
 | ||
Hemosiderosis (AmE) or haemosiderosis (BrE) is a form of iron overload disorder resulting in the accumulation of hemosiderin.
Contents
Types include:
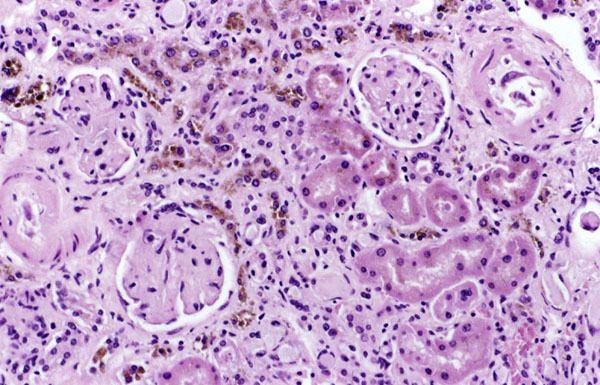
Hemosiderin deposition in the lungs is often seen after diffuse alveolar hemorrhage, which occurs in diseases such as Goodpasture's syndrome, granulomatosis with polyangiitis, and idiopathic pulmonary hemosiderosis. Mitral stenosis can also lead to pulmonary hemosiderosis. Hemosiderin collects throughout the body in hemochromatosis. Hemosiderin deposition in the liver is a common feature of hemochromatosis and is the cause of liver failure in the disease. Selective iron deposition in the beta cells of pancreatic islets leads to diabetes due to distribution of transferrin receptor on the beta cells of islets and in the skin leads to hyperpigmentation. Hemosiderin deposition in the brain is seen after bleeds from any source, including chronic subdural hemorrhage, cerebral arteriovenous malformations, cavernous hemangiomata. Hemosiderin collects in the skin and is slowly removed after bruising; hemosiderin may remain in some conditions such as stasis dermatitis. Hemosiderin in the kidneys has been associated with marked hemolysis and a rare blood disorder called paroxysmal nocturnal hemoglobinuria.
Hemosiderin may deposit in diseases associated with iron overload. These diseases are typically diseases in which chronic blood loss requires frequent blood transfusions, such as sickle cell anemia and thalassemia, though beta thalassemia minor has been associated with hemosiderin deposits in the liver in those with non-alcoholic fatty liver disease independent of any transfusions.
Treatment
Treatment for hemosiderin focuses on limiting the effects of the underlying disease leading to continued deposition. In hemochromatosis, this entails frequent phlebotomy granulomatosis, immune suppression is required. Limiting blood transfusions and institution of iron chelation therapy when iron overload is detected are important when managing sickle-cell anemia and other chronic hemolytic anemias.
Diagnosis
There are several methods available for diagnosing and monitoring hemosiderosis including:
Serum ferritin is a low cost, readily available, and minimally invasive method for assessing body iron stores. However, the major problem with using it as an indicator of hemosiderosis is that it can be elevated in a range of other medical conditions unrelated to iron levels including infection, inflammation, fever, liver disease, renal disease and cancer.
While liver biopsies provide a direct measure of liver iron concentration, the small sample size relative to the size of the liver can lead to sampling errors given the heterogeneity of iron concentration within the liver. Furthermore, the invasive nature of liver biopsy and the associated risks of complications (which can range from pain, haemorrhage, gallbladder perforation and other morbidities through to death in approx 1 in 10,000 cases) prevent it being used as a regular monitoring tool.
MRI is emerging as an alternative method for measuring liver iron loading because it is non-invasive, safer and generally cheaper to perform than liver biopsy; does not suffer from problems with sampling variability; and can be used more frequently than performing liver biopsies.