
ICD-9-CM 275.03 MedlinePlus 000327 | ICD-10 E83.1 DiseasesDB 5581 | |
 | ||
Synonyms bronze diabetes, hemochromatosis, haemochromatosis | ||
Iron overload, also known as hemochromatosis, indicates accumulation of iron in the body from any cause. The most important causes are hereditary haemochromatosis (HHC), a genetic disorder, and transfusional iron overload, which can result from repeated blood transfusions.
Contents
Signs and symptoms
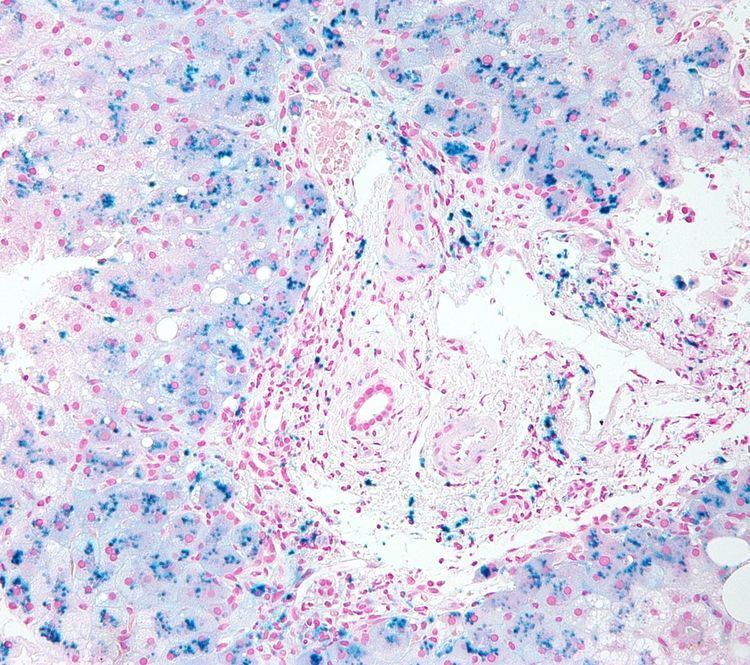
Organs commonly affected by haemochromatosis are the liver, heart, and endocrine glands.
Haemochromatosis may present with the following clinical syndromes:
Causes
The causes can be distinguished between primary cases (hereditary or genetically determined) and less frequent secondary cases (acquired during life). People of Celtic (Irish, Scottish, Welsh, Cornish, Breton etc.), English, and Scandinavian origin have a particularly high incidence of whom about 10% are carriers of the C282Y mutation on the HFE gene associated with HLA-A3 and 1% suffer from the condition.
Primary haemochromatosis
Although it was known most of the 20th century that most cases of haemochromatosis were inherited, they were incorrectly assumed to depend on a single gene. The overwhelming majority depend on mutations of the HFE gene discovered in 1996, but since then others have been discovered and sometimes are grouped together as "non-classical hereditary haemochromatosis", "non-HFE related hereditary haemochromatosis", or "non-HFE haemochromatosis".
Most types of hereditary haemochromatosis have autosomal recessive inheritance, while type 4 has autosomal dominant inheritance.
Secondary haemochromatosis
Diagnosis
There are several methods available for diagnosing and monitoring iron loading including:
Serum ferritin testing is a low-cost, readily available, and minimally invasive method for assessing body iron stores. However, the major problem with using it as an indicator of iron overload is that it can be elevated in a range of other medical conditions unrelated to iron levels including infection, inflammation, fever, liver disease, kidney disease, and cancer. Also, total iron binding capacity may be low, but can also be normal.
The standard of practice in diagnosis of haemochromatosis was recently reviewed by Pietrangelo. Positive HFE analysis confirms the clinical diagnosis of haemochromatosis in asymptomatic individuals with blood tests showing increased iron stores, or for predictive testing of individuals with a family history of haemochromatosis. The alleles evaluated by HFE gene analysis are evident in ~80% of patients with haemochromatosis; a negative report for HFE gene does not rule out haemochromatosis. In a patient with negative HFE gene testing, elevated iron status for no other obvious reason, and family history of liver disease, additional evaluation of liver iron concentration is indicated. In this case, diagnosis of haemochromatosis is based on biochemical analysis and histologic examination of a liver biopsy. Assessment of the hepatic iron index (HII) is considered the "gold standard" for diagnosis of haemochromatosis.
Magnetic resonance imaging (MRI) is emerging as a noninvasive alternative to accurately estimate iron deposition levels in the liver as well as heart, joints, and pituitary gland.
Screening
Family members of those with primary haemochromatosis should be screened to determine if they are a carrier or if they could develop the disease. This can allow preventive measures to be taken.
Screening the general population is not recommended.
Treatment
Routine treatment in an otherwise-healthy person consists of regularly scheduled phlebotomies (bloodletting or erythrocytapheresis). When first diagnosed, the phlebotomies may be fairly frequent, until iron levels can be brought to within normal range. Once iron and other markers are within the normal range, treatments may be scheduled every other month or every three months depending upon the underlying cause of the iron overload and the person's iron load. A phlebotomy session typically draws between 450 to 500 cc whole blood.
For those unable to tolerate routine blood draws, there is a chelating agent available for use. The drug deferoxamine binds with iron in the bloodstream and enhances its elimination in urine and faeces. Typical treatment for chronic iron overload requires subcutaneous injection over a period of 8–12 hours daily. Two newer iron chelating drugs that are licensed for use in patients receiving regular blood transfusions to treat thalassaemia (and, thus, who develop iron overload as a result) are deferasirox and deferiprone.
Prognosis
Affected individuals over age 40 or who have high serum ferritin levels are at risk for developing cirrhosis. Iron overload increases the risk of hepatocellular carcinoma. This risk is greater in those with cirrhosis but is still present in those without cirrhosis. Significant problems occur in around one in ten.
Epidemiology
It is most common in certain European populations (such as the Irish and Norwegians) and occurs in 0.6% of the population. Men with the disease are 24 times more likely to experience symptoms than affected women.
Terminology
Historically, the term haemochromatosis (spelled hemochromatosis in American English) was initially used to refer to what is now more specifically called haemochromatosis type 1 (or HFE-related hereditary haemochromatosis). Currently, haemochromatosis (without further specification) is mostly defined as iron overload with a hereditary/primary cause, or originating from a metabolic disorder. However, the term is currently also used more broadly to refer to any form of iron overload, thus requiring specification of the cause, for example, hereditary haemochromatosis. Hereditary haemochromatosis is an autosomal recessive disorder with estimated prevalence in the population of 1 in 200 among patients with European ancestry, with lower incidence in other ethnic groups. The gene responsible for hereditary haemochromatosis (known as HFE gene) is located on chromosome 6; the majority of hereditary haemochromatosis patients have mutations in this HFE gene.
Hereditary haemochromatosis is characterized by an accelerated rate of intestinal iron absorption and progressive iron deposition in various tissues. This typically begins to be expressed in the third to fifth decades of life, but may occur in children. The most common presentation is hepatic (liver) cirrhosis in combination with hypopituitarism, cardiomyopathy, diabetes, arthritis, or hyperpigmentation. Because of the severe sequelae of this disorder if left untreated, and recognizing that treatment is relatively simple, early diagnosis before symptoms or signs appear is important.
In general, the term haemosiderosis is used to indicate the pathological effect of iron accumulation in any given organ, which mainly occurs in the form of the iron-storage complex haemosiderin. Sometimes, the simpler term siderosis is used instead.
Other definitions distinguishing haemochromatosis or haemosiderosis that are occasionally used include: